

Features of Postpartum Hemorrhage-Associated Thrombotic Microangiopathy and Role of Short-Term Complement Inhibition
- PMID: 38765599
- PMCID: PMC11101778
- DOI: 10.1016/j.ekir.2024.01.035
Features of Postpartum Hemorrhage-Associated Thrombotic Microangiopathy and Role of Short-Term Complement Inhibition
Erratum in
-
Erratum to "Features of Postpartum Hemorrhage-Associated Thrombotic Microangiopathy and Role of Short-Term Complement Inhibition" [Kidney International Reports Volume 9, Issue 4, April 2024, Pages 919-928].Kidney Int Rep. 2024 Aug 6;9(10):3081. doi: 10.1016/j.ekir.2024.08.001. eCollection 2024 Oct. Kidney Int Rep. 2024. PMID: 39430175 Free PMC article.
Abstract
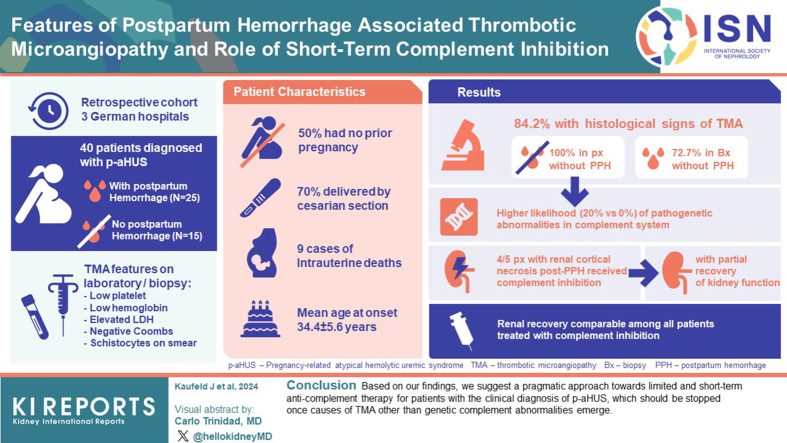
Introduction: In pregnancy-related atypical hemolytic uremic syndrome (p-aHUS), transferring recommendations for treatment decisions from nonpregnant cohorts with thrombotic microangiopathy (TMA) is difficult. Although potential causes of p-aHUS may be unrelated to inherent complement defects, peripartal complications such as postpartum hemorrhage (PPH) or (pre)eclampsia or Hemolysis, Elevated Liver enzymes and Low Platelets (HELLP) syndrome may be unrecognized drivers of complement activation.
Methods: To evaluate diagnostic and therapeutic decisions in the practical real-life setting, we conducted an analysis of a cohort of 40 patients from 3 German academic hospitals with a diagnosis of p-aHUS, stratified by the presence (n = 25) or absence (n = 15) of PPH.
Results: Histological signs of TMA were observed in 84.2% of all patients (100% vs. 72.7% in patients without or with PPH, respectively). Patients without PPH had a higher likelihood (20% vs. 0%) of pathogenic genetic abnormalities in the complement system although notably less than in other published cohorts. Four of 5 patients with observed renal cortical necrosis (RCN) after PPH received complement inhibition and experienced partially recovered kidney function. Patients on complement inhibition with or without PPH had an increased need for kidney replacement therapy (KRT) and plasma exchange (PEX). Because renal recovery was comparable among all patients treated with complement inhibition, a potential beneficial effect in this group of pregnancy-associated TMAs and p-aHUS is presumed.
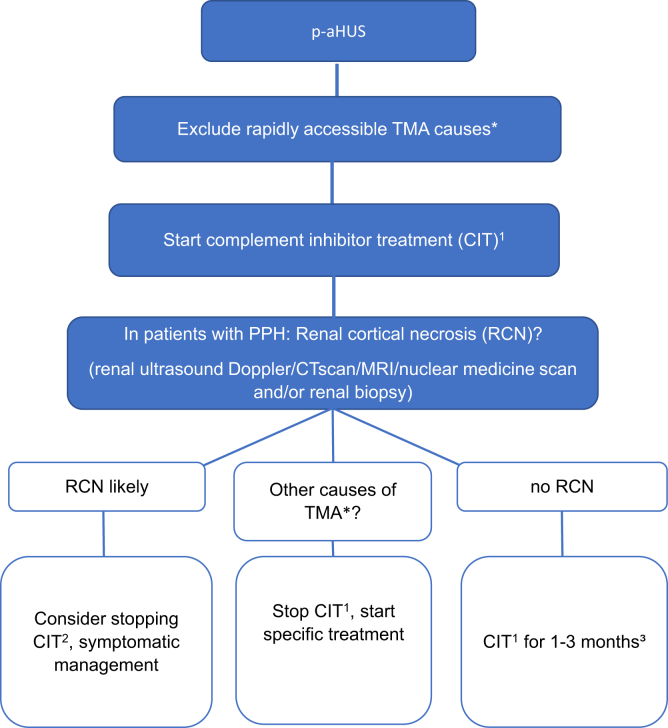
Conclusion: Based on our findings, we suggest a pragmatic approach toward limited and short-term anticomplement therapy for patients with a clinical diagnosis of p-aHUS, which should be stopped once causes of TMA other than genetic complement abnormalities emerge.
Keywords: complement inhibition; genetic kidney disease; p-aHUS; postpartum hemorrhage; pregnancy; renal cortical necrosis.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures
References
-
- Delmas Y., Helou S., Chabanier P., et al. Incidence of obstetrical thrombotic thrombocytopenic purpura in a retrospective study within thrombocytopenic pregnant women. A difficult diagnosis and a treatable disease. BMC Pregnancy Childbirth. 2015;15:137. doi: 10.1186/s12884-015-0557-5. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
