

Case Reports
doi: 10.1016/j.case.2024.01.004.
eCollection 2024 Apr.
Cor Triatriatum Dexter and Right Atrial Mass Causing Severe Inflow Obstruction
Affiliations
- PMID: 38765628
- PMCID: PMC11096656
- DOI: 10.1016/j.case.2024.01.004
Item in Clipboard
Case Reports
Cor Triatriatum Dexter and Right Atrial Mass Causing Severe Inflow Obstruction
CASE (Phila).
.
No abstract available
Keywords: Antiphospholipid syndrome; Cardiac mass; Cor triatriatum; Systemic lupus erythematosus; Tricuspid valve inflow obstruction.
Figures


(A) Twelve-lead electrocardiogram demonstrates normal sinus rhythm, rightward axis, right atrial abnormality, and poor R-wave progression. (B) Anteroposterior and lateral chest radiography demonstrates normal cardiac silhouette with no apparent calcifications, normal great vessels, normal pulmonary parenchyma, and elevated right hemidiaphragm.
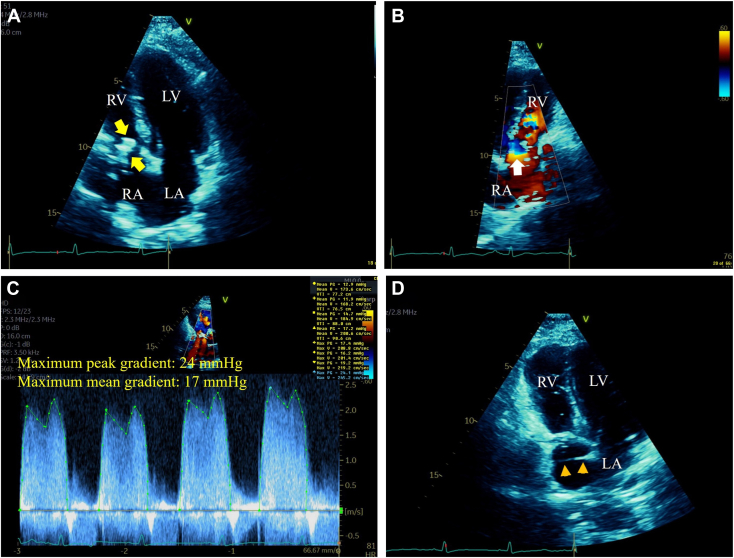
(A) Two-dimensional TTE, apical 4-chamber view, during mid-diastole, demonstrates a large (2.5 × 1.5 cm), elongated, irregular, and hyperreflectant RA mass moving inferiorly into the TV inflow (arrows). (B) Two-dimensional TTE, reversed apical 4-chamber view with color-flow Doppler during late diastole, demonstrates nonturbulent flow within the RA cavity, in contrast to turbulent flow with a convergence zone (arrow) at the TV inflow level caused by the obstructive RA mass. (C) Two-dimensional TTE, short-axis view, color flow–guided continuous-wave Doppler, demonstrates severe TV inflow obstruction with maximum peak and mean gradients of 24 mm Hg and 17 mm Hg, respectively. (D) Two-dimensional TTE, apical 4-chamber view, during early systole, demonstrates a membrane traversing the RA cavity from the lateral wall to the IAS (arrowheads) suggestive of a CTD. LV, Left ventricle; RV, right ventricle.

Pulmonary perfusion scan with multiple rotational views demonstrates normal perfusion indicative of low probability of chronic pulmonary thromboembolism.

(A) Two-dimensional TEE, midesophageal biplane (0°, left; 90°, right) views during mid-diastole, demonstrates a large (3.3 × 1.5 × 1.1 cm), elongated, and heterogeneously echoreflectant RA mass (arrows) moving inferiorly into the TV inflow causing obstruction and a linear, homogeneously echoreflectant, and nonmobile membrane (arrowheads) with an aperture of 1.2 cm (double-headed arrow) dividing the RA into a superior and inferior chamber. Associated posterior tricuspid annular calcification (green arrows) is also noted. In addition, RA dilatation and bowing IAS toward the LA (orange arrows) indicative of high RA pressure is noted. (B) Two-dimensional TEE, midesophageal 4-chamber (22°) view during midsystole, demonstrates the large RA mass moving superiorly (arrow), the dividing atrial membrane extending from the RA lateral wall to the IAS (arrowheads), and a small, oval, soft tissue echoreflectant mass (orange arrow) adherent to the atrial side of the calcified annulus (green arrow). LV, Left ventricle; RV, right ventricle.
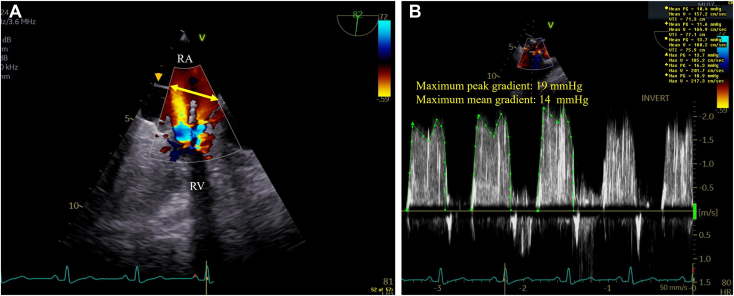
(A) Two-dimensional TEE, midesophageal right heart–oriented (82°) view with color-flow Doppler during late diastole, demonstrates the dividing RA membrane (arrowhead) with a large (2.0 cm) aperture (double-headed arrow) with nonturbulent flow at this level, in contrast to turbulent flow at the TV inflow level (arrows) caused by the obstructive mass. (B) Two-dimensional TEE, midesophageal right heart–oriented (82°) view with color-flow Doppler-guided continuous-wave Doppler, demonstrates severe TV inflow obstruction with maximum peak and mean gradients of 19 mm Hg and 14 mm Hg, respectively (at a heart rate of 80 bpm). RV, Right ventricle.

Three-dimensional TEE with a superior to inferior RA view demonstrates the large RA mass (thick arrows) attached to the anterolateral free wall by a short stalk (thin arrow) moving superiorly during systole (A) and inferiorly into the TV inflow during diastole (B). Peripheral portions of the dividing membrane are also noted attached circumferentially to the RA walls (arrowheads).
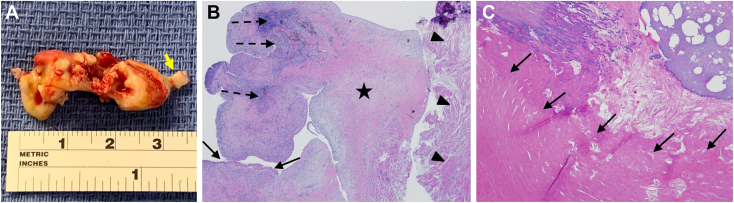
(A) Gross pathology demonstrates that the large (3.5 × 1.5 × 1.0 cm) RA mass is elongated, multilobed, irregular, and with a short stalk (arrow). (B) Histopathology demonstrates a predominantly old thrombus adherent to the atrial muscle (arrowheads) with areas of early organization with mild chronic inflammation (dashed arrows), areas of denser fibrosis (star), and a cap of fresh fibrin thrombus (arrows). (C) The small mass from the tricuspid annulus demonstrates a layered bright pink eosinophilic acute or subacute thrombus (arrows).
References
-
- Jha A.K., Makhija N. Cor triatriatum: a review. Semin Cardiothorac Vasc Anesth. 2017;21:178–185. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous
