

This is a preprint.
Neutrophil percentages in bronchoalveolar lavage fluid: Implications for diagnosing bacterial pneumonia in patients with immunocompromise and neutropenia
- PMID: 38766045
- PMCID: PMC11100846
- DOI: 10.1101/2024.05.04.24306709
Neutrophil percentages in bronchoalveolar lavage fluid: Implications for diagnosing bacterial pneumonia in patients with immunocompromise and neutropenia
Abstract
Rationale: Pneumonia is the most common infection in ICU patients and a leading cause for death. Assessment of bronchoalveolar lavage fluid (BALF) cellularity can aid in pneumonia diagnosis. Low percentages (<50%) of BALF neutrophils have a high negative predictive value for bacterial pneumonia in a general medical ICU population. The operating characteristics in patients with immunocompromise and neutropenia are less clear.
Objective: To compare BALF % neutrophils operating characteristics in patients with and without immunocompromise or neutropenia.
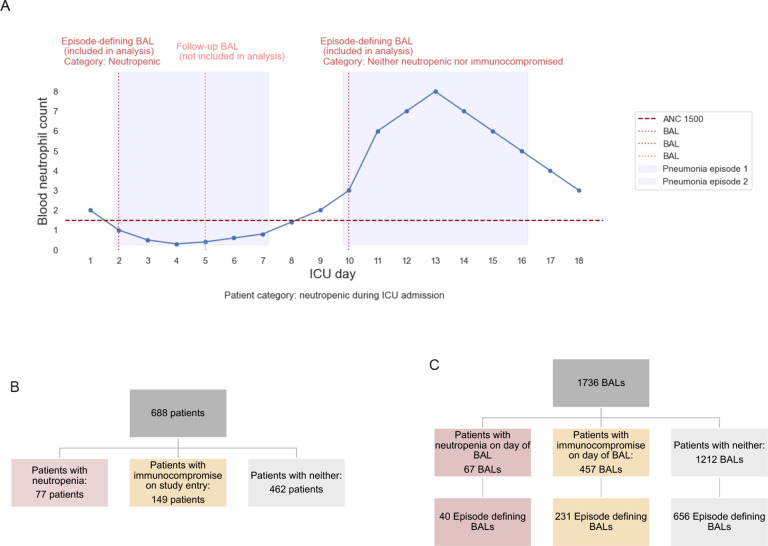
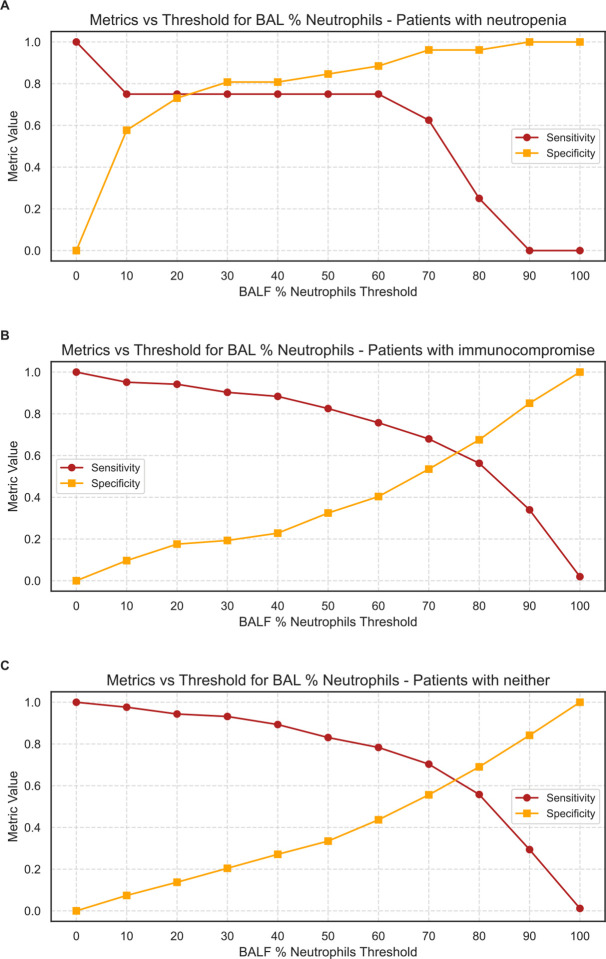
Methods: This was a single center observational cohort study. Patients were categorized into three groups: (1) patients with neutropenia, (2) patients with underlying immunocompromise, and (3) patients with neither. BAL-level analysis reflected neutropenia and immunocompromise state on day of BAL sampling. Operating characteristics of BALF % neutrophils were calculated using varying thresholds of alveolar neutrophilia. Median [Q1,Q3] are reported for nonparametric data and compared using Mann-Whitney U tests.
Results: 688 mechanically ventilated patients had 1736 BAL samples. Among bacterial pneumonia episodes, no difference was found in BALF % neutrophils between patients with underlying immunocompromise and patients with neither neutropenia nor immunocompromise on day of sampling: 82.0% [61.0, 91.0] vs 81.0% [66.0, 91.0], p=0.859. However, when neutropenic on day of sampling, the median BALF % neutrophils was 35.0% [8.8, 67.5] (p<0.001 compared with other categories). In patients with neutropenia, a BALF % neutrophil threshold of 7% had a sensitivity of 90% for excluding bacterial pneumonia.
Conclusions: We found that among patients with bacterial pneumonia, BALF % neutrophil was not significantly lower in patients with a broad spectrum of immunocompromised states but was significantly lower when measured during acute neutropenia. We found varying thresholds of BALF % neutrophils across the three groups. Patients with neutropenia who mount even a low percent of alveolar neutrophils should raise concern for bacterial pneumonia.
Keywords: alveolar neutrophilia; bronchoalveolar lavage fluid analysis; chest infections; host response; immunocompromise; neutropenia; pneumonia.
Conflict of interest statement
Declarations of interests: BDS holds US patent 10,905,706, “Compositions and methods to accelerate resolution of acute lung inflammation,” and serves on the scientific advisory board of Zoe Biosciences, in which he holds stock options. Other authors have no conflicts within the area of this work.
Figures

Similar articles
-
Comparison of Two Modern Survival Prediction Tools, SORG-MLA and METSSS, in Patients With Symptomatic Long-bone Metastases Who Underwent Local Treatment With Surgery Followed by Radiotherapy and With Radiotherapy Alone.Clin Orthop Relat Res. 2024 Dec 1;482(12):2193-2208. doi: 10.1097/CORR.0000000000003185. Epub 2024 Jul 23. Clin Orthop Relat Res. 2024. PMID: 39051924
-
Bronchoscopy-guided antimicrobial therapy for cystic fibrosis.Cochrane Database Syst Rev. 2024 May 3;5(5):CD009530. doi: 10.1002/14651858.CD009530.pub5. Cochrane Database Syst Rev. 2024. PMID: 38700027 Free PMC article.
-
Signs and symptoms to determine if a patient presenting in primary care or hospital outpatient settings has COVID-19.Cochrane Database Syst Rev. 2022 May 20;5(5):CD013665. doi: 10.1002/14651858.CD013665.pub3. Cochrane Database Syst Rev. 2022. PMID: 35593186 Free PMC article.
-
Prophylactic antibiotics or G(M)-CSF for the prevention of infections and improvement of survival in cancer patients receiving myelotoxic chemotherapy.Cochrane Database Syst Rev. 2015 Dec 21;2015(12):CD007107. doi: 10.1002/14651858.CD007107.pub3. Cochrane Database Syst Rev. 2015. PMID: 26687844 Free PMC article.
-
Very early discharge versus early discharge versus non-early discharge in children with cancer and febrile neutropenia.Cochrane Database Syst Rev. 2016 Feb 22;2(2):CD008382. doi: 10.1002/14651858.CD008382.pub2. Cochrane Database Syst Rev. 2016. PMID: 26899263 Free PMC article.
References
-
- Troeger C, Forouzanfar M, Rao PC, et al. Estimates of the global, regional, and national morbidity, mortality, and aetiologies of lower respiratory tract infections in 195 countries: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Infect Dis. 2017;17(11):1133–1161. doi:10.1016/S1473-3099(17)30396-1 - DOI - PMC - PubMed
Publication types
Grants and funding
- R01 HL153122/HL/NHLBI NIH HHS/United States
- U19 AI181102/AI/NIAID NIH HHS/United States
- K23 HL169815/HL/NHLBI NIH HHS/United States
- U19 AI135964/AI/NIAID NIH HHS/United States
- P01 HL154998/HL/NHLBI NIH HHS/United States
- U01 TR003528/TR/NCATS NIH HHS/United States
- R01 LM013337/LM/NLM NIH HHS/United States
- R01 HL147290/HL/NHLBI NIH HHS/United States
- R01 HL147575/HL/NHLBI NIH HHS/United States
- R01 HL149883/HL/NHLBI NIH HHS/United States
- P01 AG049665/AG/NIA NIH HHS/United States
- 24PRE1196998/AHA/American Heart Association-American Stroke Association/United States
LinkOut - more resources
Full Text Sources