

This is a preprint.
Naturalistic acute pain states decoded from neural and facial dynamics
- PMID: 38766098
- PMCID: PMC11100805
- DOI: 10.1101/2024.05.10.593652
Naturalistic acute pain states decoded from neural and facial dynamics
Update in
-
Naturalistic acute pain states decoded from neural and facial dynamics.Nat Commun. 2025 May 11;16(1):4371. doi: 10.1038/s41467-025-59756-5. Nat Commun. 2025. PMID: 40350488 Free PMC article.
Abstract
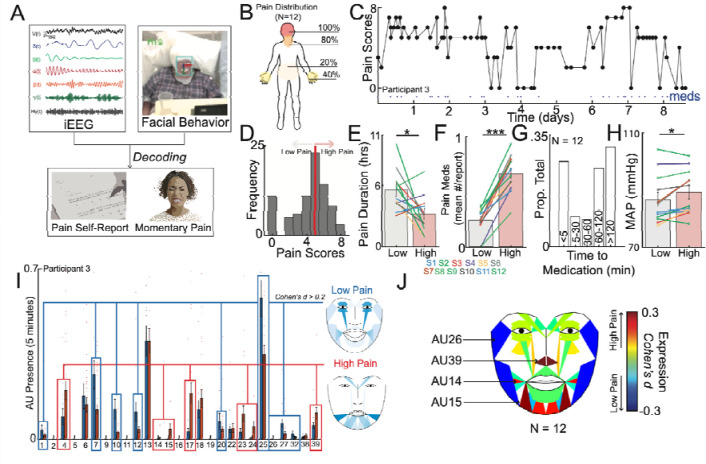
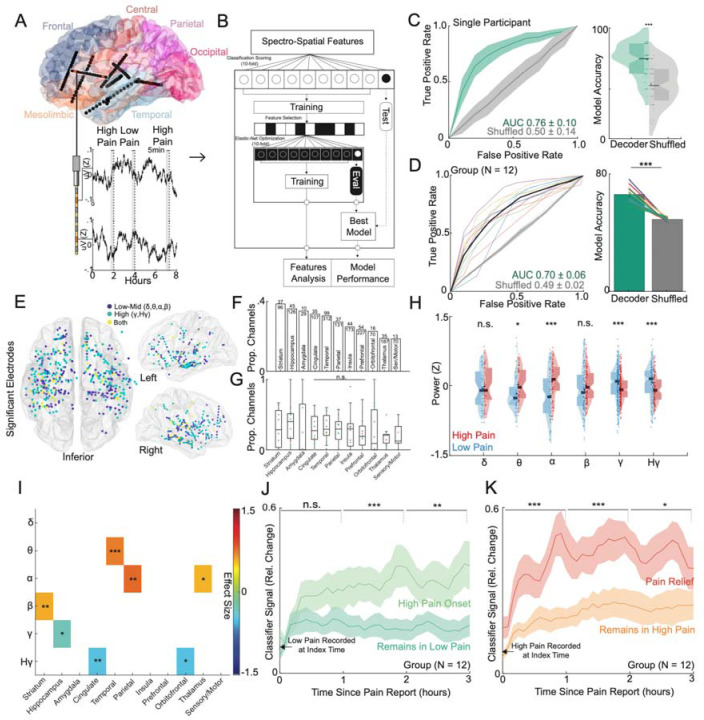
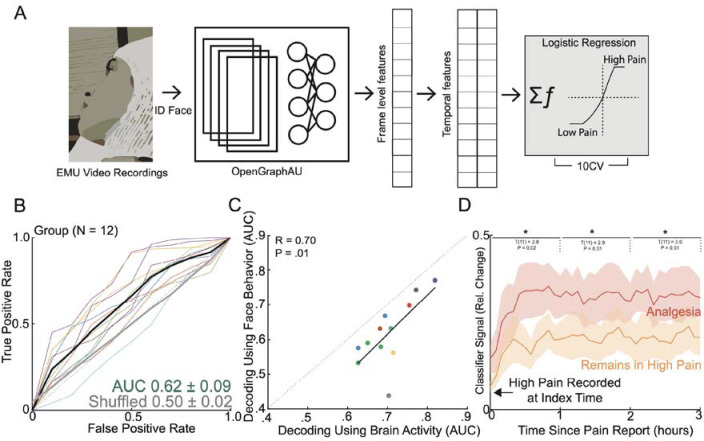
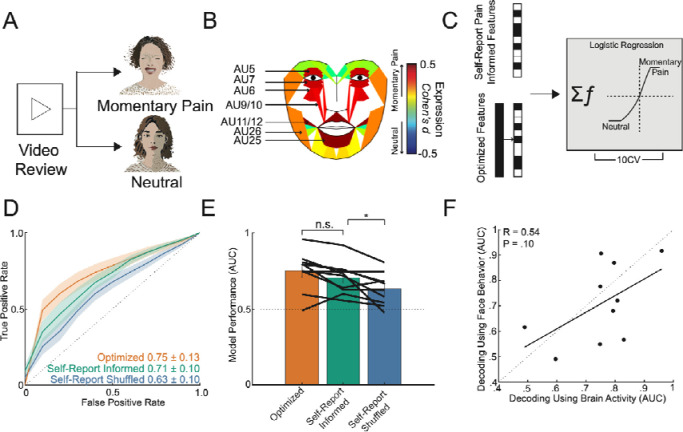
Pain is a complex experience that remains largely unexplored in naturalistic contexts, hindering our understanding of its neurobehavioral representation in ecologically valid settings. To address this, we employed a multimodal, data-driven approach integrating intracranial electroencephalography, pain self-reports, and facial expression quantification to characterize the neural and behavioral correlates of naturalistic acute pain in twelve epilepsy patients undergoing continuous monitoring with neural and audiovisual recordings. High self-reported pain states were associated with elevated blood pressure, increased pain medication use, and distinct facial muscle activations. Using machine learning, we successfully decoded individual participants' high versus low self-reported pain states from distributed neural activity patterns (mean AUC = 0.70), involving mesolimbic regions, striatum, and temporoparietal cortex. High self-reported pain states exhibited increased low-frequency activity in temporoparietal areas and decreased high-frequency activity in mesolimbic regions (hippocampus, cingulate, and orbitofrontal cortex) compared to low pain states. This neural pain representation remained stable for hours and was modulated by pain onset and relief. Objective facial expression changes also classified self-reported pain states, with results concordant with electrophysiological predictions. Importantly, we identified transient periods of momentary pain as a distinct naturalistic acute pain measure, which could be reliably differentiated from affect-neutral periods using intracranial and facial features, albeit with neural and facial patterns distinct from self-reported pain. These findings reveal reliable neurobehavioral markers of naturalistic acute pain across contexts and timescales, underscoring the potential for developing personalized pain interventions in real-world settings.
Figures
Similar articles
-
Naturalistic acute pain states decoded from neural and facial dynamics.Nat Commun. 2025 May 11;16(1):4371. doi: 10.1038/s41467-025-59756-5. Nat Commun. 2025. PMID: 40350488 Free PMC article.
-
Decoding naturalistic affective behaviour from spectro-spatial features in multiday human iEEG.Nat Hum Behav. 2022 Jun;6(6):823-836. doi: 10.1038/s41562-022-01310-0. Epub 2022 Mar 10. Nat Hum Behav. 2022. PMID: 35273355 Free PMC article.
-
Neural dynamics between anterior insular cortex and right supramarginal gyrus dissociate genuine affect sharing from perceptual saliency of pretended pain.Elife. 2021 Aug 19;10:e69994. doi: 10.7554/eLife.69994. Elife. 2021. PMID: 34409940 Free PMC article.
-
Stereotactic electroencephalography in epilepsy patients for mapping of neural circuits related to emotional and psychiatric behaviors: a systematic review.Neurosurg Focus. 2023 Feb;54(2):E4. doi: 10.3171/2022.11.FOCUS22615. Neurosurg Focus. 2023. PMID: 36724521
-
Towards an ecologically valid naturalistic cognitive neuroscience of memory and event cognition.Neuropsychologia. 2024 Oct 10;203:108970. doi: 10.1016/j.neuropsychologia.2024.108970. Epub 2024 Aug 13. Neuropsychologia. 2024. PMID: 39147361 Review.
References
-
- Čeko M., Kragel P. A., Woo C.-W., López-Solà M. & Wager T. D. Common and stimulus-type-specific brain representations of negative affect. Nat. Neurosci. 25, 760–770 (2022). - PubMed
-
- Picard M.-E. et al. Facial expression is a distinctive behavioural marker of pain processing in the brain. bioRxiv (2023) doi:10.1101/2023.07.26.550504. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources