

This is a preprint.
Radiomics-Based Predictive Nomogram for Assessing the Risk of Intracranial Aneurysms
- PMID: 38766264
- PMCID: PMC11100888
- DOI: 10.21203/rs.3.rs-4350156/v1
Radiomics-Based Predictive Nomogram for Assessing the Risk of Intracranial Aneurysms
Update in
-
Radiomics-Based Predictive Nomogram for Assessing the Risk of Intracranial Aneurysms.Transl Stroke Res. 2025 Feb;16(1):79-87. doi: 10.1007/s12975-024-01268-3. Epub 2024 Jul 2. Transl Stroke Res. 2025. PMID: 38954365
Abstract
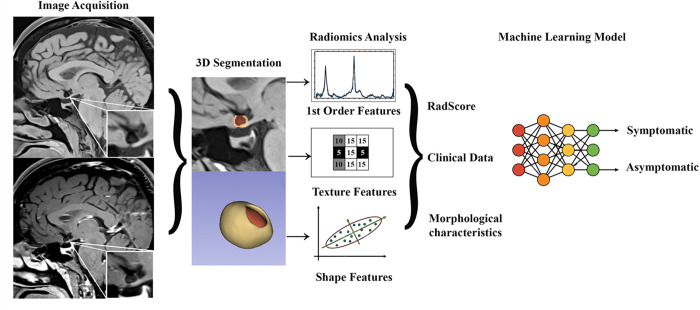
Background: Aneurysm wall enhancement (AWE) has the potential to be used as an imaging biomarker for the risk stratification of intracranial aneurysms (IAs). Radiomics provides a refined approach to quantify and further characterize AWE's textural features. This study examines the performance of AWE quantification combined with clinical information in detecting symptomatic IAs.
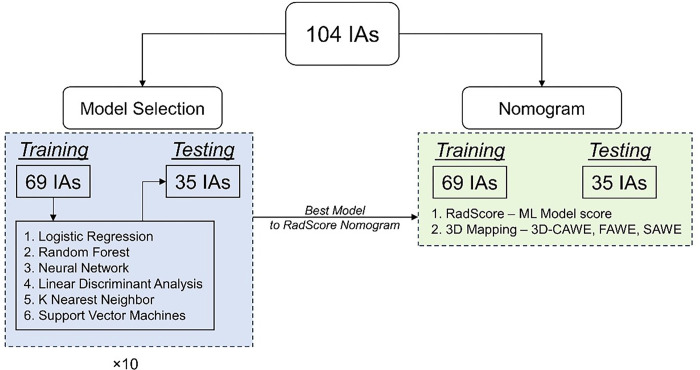
Methods: Ninety patients harboring 104 IAs (29 symptomatic and 75 asymptomatic) underwent high-resolution magnetic resonance imaging (HR-MRI). The assessment of AWE was performed using two different methods: 3D-AWE mapping and composite radiomics-based score (RadScore). The dataset was split into training and testing subsets. The testing set was used to build two different nomograms using each modality of AWE assessment combined with patients' demographic information and aneurysm morphological data. Finally, each nomogram was evaluated on an independent testing set.
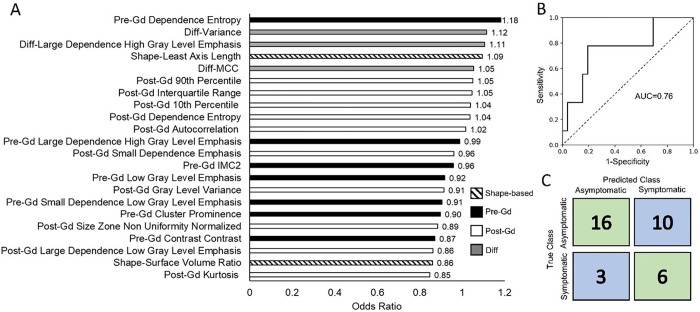
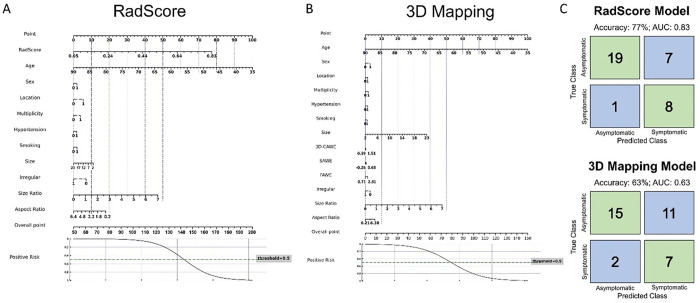
Results: A total of 22 radiomic features were significantly different between symptomatic and asymptomatic IAs. The 3D-AWE Mapping nomogram achieved an area under the curve (AUC) of 0.77 (63% accuracy, 78% sensitivity and 58% specificity). The RadScore nomogram exhibited a better performance, achieving an AUC of 0.83 (77% accuracy, 89% sensitivity and 73% specificity).
Conclusions: Combining AWE quantification through radiomic analysis with patient demographic data in a clinical nomogram achieved high accuracy in detecting symptomatic IAs.
Keywords: Aneurysms; aneurysm wall enhancement; radiomics.
Figures
References
-
- Sanchez S, Hickerson M, Patel RR, Ghazaleh D, Tarchand R, Paranjape GS et al. Morphological Characteristics of Ruptured Brain Aneurysms: A Systematic Literature Review and Meta-Analysis. Stroke: Vascular and Interventional Neurology. 2023;3(2):e000707. doi:doi:10.1161/SVIN.122.000707. - DOI
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
