

Tuberculosis-diabetes comorbidities: Mechanistic insights for clinical considerations and treatment challenges
- PMID: 38766427
- PMCID: PMC11099355
- DOI: 10.4239/wjd.v15.i5.853
Tuberculosis-diabetes comorbidities: Mechanistic insights for clinical considerations and treatment challenges
Abstract
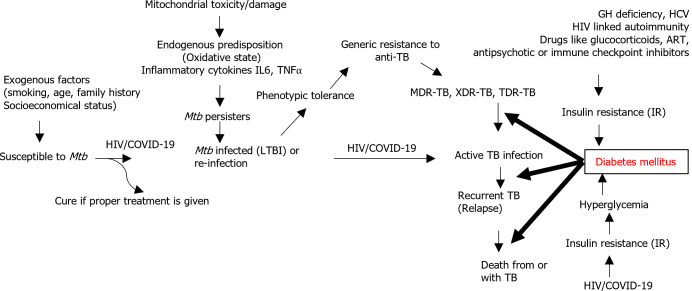
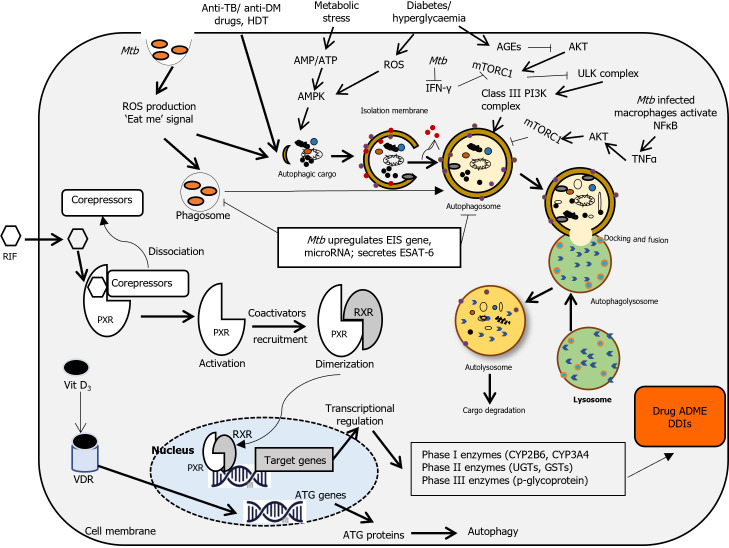
Tuberculosis (TB) remains a leading cause of death among infectious diseases, particularly in poor countries. Viral infections, multidrug-resistant and ex-tensively drug-resistant TB strains, as well as the coexistence of chronic illnesses such as diabetes mellitus (DM) greatly aggravate TB morbidity and mortality. DM [particularly type 2 DM (T2DM)] and TB have converged making their control even more challenging. Two contemporary global epidemics, TB-DM behaves like a syndemic, a synergistic confluence of two highly prevalent diseases. T2DM is a risk factor for developing more severe forms of multi-drug resistant-TB and TB recurrence after preventive treatment. Since a bidirectional relationship exists between TB and DM, it is necessary to concurrently treat both, and promote recommendations for the joint management of both diseases. There are also some drug-drug interactions resulting in adverse treatment outcomes in TB-DM patients including treatment failure, and reinfection. In addition, autophagy may play a role in these comorbidities. Therefore, the TB-DM comorbidities present several health challenges, requiring a focus on multidisciplinary collaboration and integrated strategies, to effectively deal with this double burden. To effectively manage the comorbidity, further screening in affected countries, more suitable drugs, and better treatment strategies are required.
Keywords: Autophagy; Coinfections; Comorbidity; Diabetes mellitus; Drug-drug interactions; Treatment challenges; Tuberculosis.
©The Author(s) 2024. Published by Baishideng Publishing Group Inc. All rights reserved.
Conflict of interest statement
Conflict-of-interest statement: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Navigating the dual burden of diabetes mellitus and tuberculosis: A comprehensive review of clinical and public health strategies.Indian J Tuberc. 2025 Apr;72(2):253-258. doi: 10.1016/j.ijtb.2025.03.011. Epub 2025 Mar 19. Indian J Tuberc. 2025. PMID: 40518222 Review.
-
Tuberculosis and diabetes mellitus: The complexity of the comorbid interactions.Int J Infect Dis. 2024 Sep;146:107140. doi: 10.1016/j.ijid.2024.107140. Epub 2024 Jun 15. Int J Infect Dis. 2024. PMID: 38885832 Review.
-
Challenges of diabetes in elderly TB patients.Indian J Tuberc. 2022;69 Suppl 2:S264-S266. doi: 10.1016/j.ijtb.2022.10.017. Epub 2022 Oct 28. Indian J Tuberc. 2022. PMID: 36400521 Free PMC article. Review.
-
Diabetes and tuberculosis syndemic in India: A narrative review of facts, gaps in care and challenges.J Diabetes. 2024 May;16(5):e13427. doi: 10.1111/1753-0407.13427. Epub 2023 Jun 8. J Diabetes. 2024. PMID: 37292055 Free PMC article. Review.
-
The effect size of type 2 diabetes mellitus on tuberculosis drug resistance and adverse treatment outcomes.Tuberculosis (Edinb). 2017 Mar;103:83-91. doi: 10.1016/j.tube.2017.01.006. Epub 2017 Jan 24. Tuberculosis (Edinb). 2017. PMID: 28237037
Cited by
-
Estimation of the Proportion and Determinants of Diabetes Mellitus Among Notified Tuberculosis Patients in Jaipur, Rajasthan, India.Cureus. 2025 Mar 10;17(3):e80319. doi: 10.7759/cureus.80319. eCollection 2025 Mar. Cureus. 2025. PMID: 40206911 Free PMC article.
-
The role of metformin in tuberculosis control among TB and diabetes mellitus comorbid individuals.Front Microbiol. 2025 Apr 25;16:1549572. doi: 10.3389/fmicb.2025.1549572. eCollection 2025. Front Microbiol. 2025. PMID: 40351311 Free PMC article. Review.
-
Enhancing metformin efficacy with cholecalciferol and taurine in diabetes therapy: Potential and limitations.World J Diabetes. 2025 Jan 15;16(1):100066. doi: 10.4239/wjd.v16.i1.100066. World J Diabetes. 2025. PMID: 39817227 Free PMC article.
-
Dual Burden of MDR-TB and COVID-19 in a Previously Treated Tuberculosis Case: Diagnostic and Therapeutic Dilemmas.Clin Case Rep. 2025 Mar 20;13(3):e70317. doi: 10.1002/ccr3.70317. eCollection 2025 Mar. Clin Case Rep. 2025. PMID: 40124205 Free PMC article.
References
-
- Luntz G. Tuberculous diabetics: the Birmingham Regional Service. Lancet. 1954;266:973–974. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
