

Distinct Clinical Endpoints of Staphylococcus aureus Bacteraemia Complicate Assessment of Outcome
- PMID: 38767234
- PMCID: PMC11426269
- DOI: 10.1093/cid/ciae281
Distinct Clinical Endpoints of Staphylococcus aureus Bacteraemia Complicate Assessment of Outcome
Abstract
Background: We aimed to test the hypothesis that development of metastatic infection represents a distinct clinical endpoint from death due to Staphylococcus aureus bacteremia (SAB).
Methods: We conducted a retrospective observational study of adults with SAB between 20 December 2019 and 23 August st2022 (n = 464). Simple logistic regression, odds ratios, and z-scores were used to compare host, clinical, and microbiologic features.
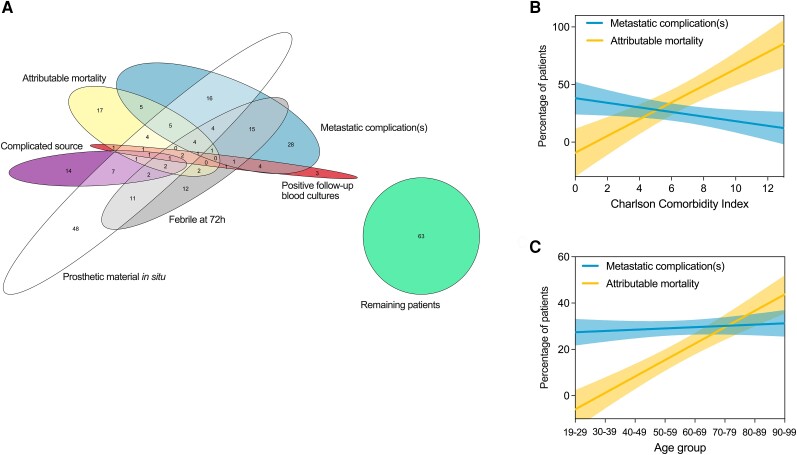
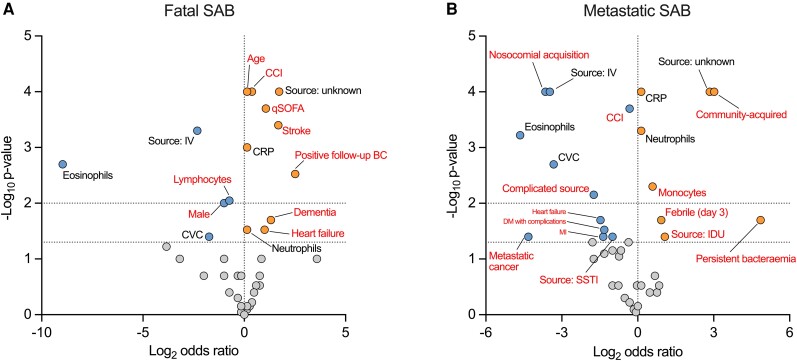
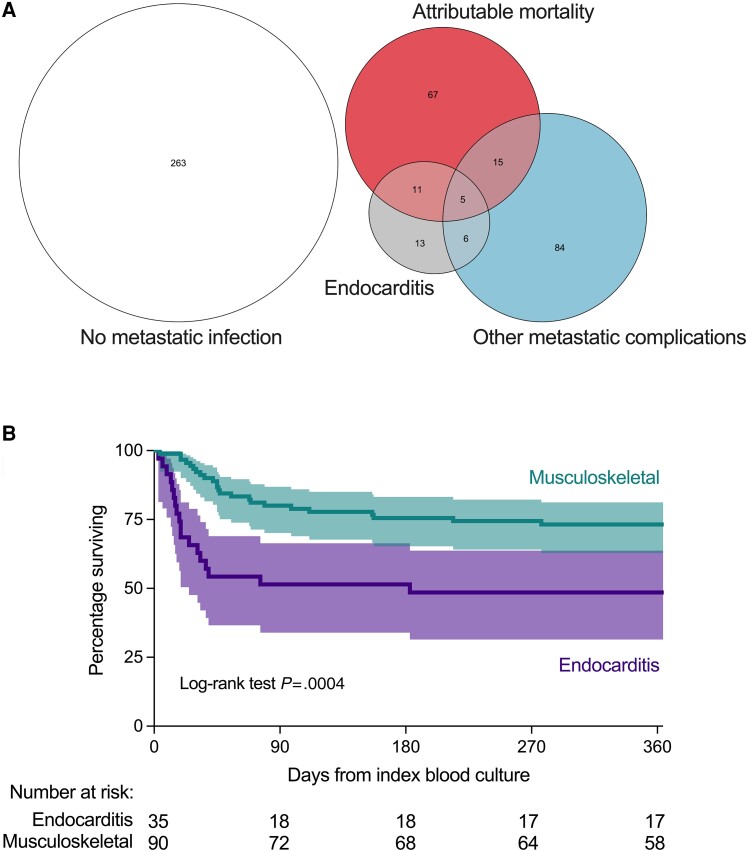
Results: Co-occurrence of attributable mortality and metastatic infection was infrequent. Charlson Comorbidity Index and age were strongly associated with attributable mortality, but not metastatic infection. We compared patients with fatal SAB (without clinically-apparent metastatic complications, 14.4% of cohort), metastatic SAB (without attributable mortality, 22.2%), neither complication (56.7%), and overlapping fatal/metastatic SAB (6.7%). Compared to SAB without complications, fatal SAB was specifically associated with older age and multi-morbidity. Metastatic SAB was specifically associated with community acquisition, persistent fever, persistent bacteremia, and recurrence. Endocarditis was over-represented in the fatal/metastatic SAB overlap group, which shared patient characteristics with fatal SAB. In contrast to other (predominantly musculoskeletal) metastatic complications, endocarditis was associated with increased mortality, with death occurring in older multi-morbid patients later after SAB onset.
Conclusions: Patients with SAB experience distinct clinical endpoints: (i) early death, associated with multi-morbidity and age; (ii) metastatic (predominantly musculoskeletal) SAB; (iii) endocarditis, associated with late death occurring in older people with multi-morbidity, and (iv) bacteraemia without complications. These distinctions could be important for selecting appropriate outcomes in clinical trials: different interventions might be required to reduce mortality versus improve clinical response in patients with metastatic SAB.
Keywords: Staphylococcus aureus; bacteraemia; clinical outcomes; clinical trials; mortality.
© The Author(s) 2024. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Conflict of interest statement
Potential conflicts of interest. V. G. F. reports grants/research support: Astra Zeneca; MedImmune; Merck; ContraFect, Karius, Genentech, Regeneron, Basilea. Paid Consultant: Astra Zeneca; GSK; Armata; Debiopharm; Genentech; Basilea Affinergy, Janssen, ContraFect, Destiny. Royalties: UpToDate. Patent pending: sepsis diagnostics. All other authors report no potential conflicts. All authors have submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest. Conflicts that the editors consider relevant to the content of the manuscript have been disclosed.
Figures
References
-
- Horino T, Hori S. Metastatic infection during Staphylococcus aureus bacteremia. J Infect Chemother 2020; 26:162–9. - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 1987; 40:373–83. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
