

Cardiovascular pathology in vasculitis
- PMID: 38767541
- PMCID: PMC11138763
- DOI: 10.32074/1591-951X-993
Cardiovascular pathology in vasculitis
Abstract
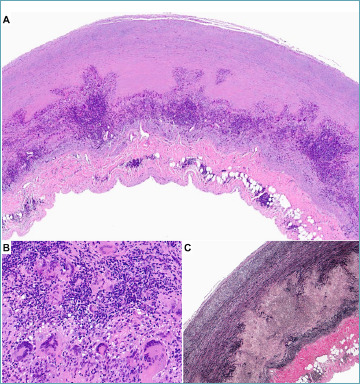
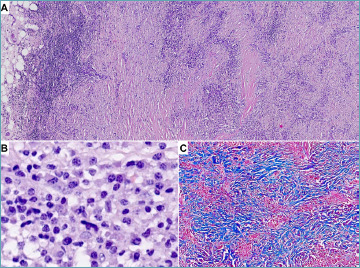
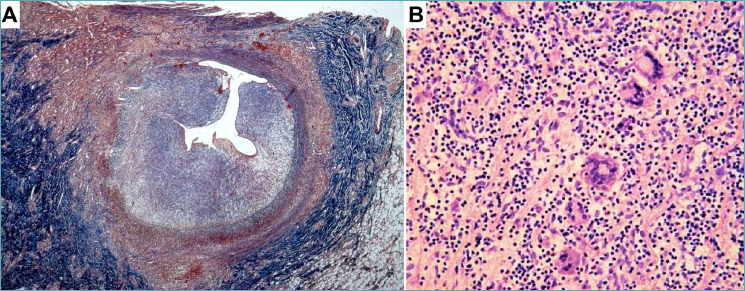
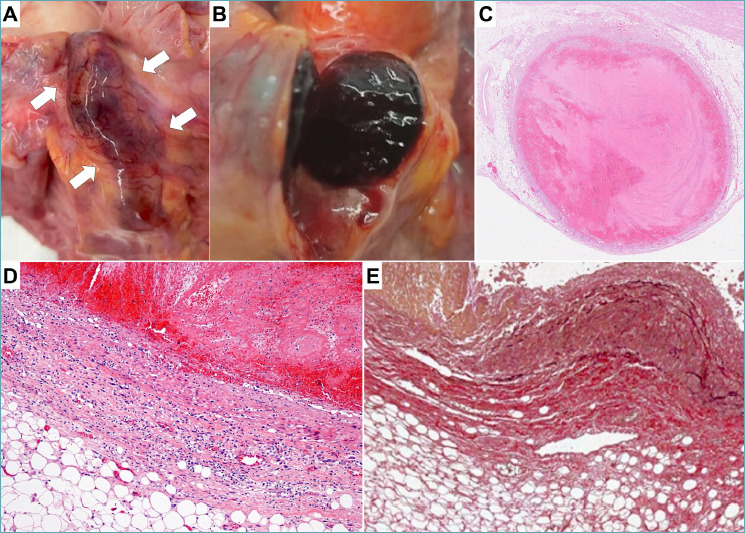
Vasculitides are diseases that can affect any vessel. When cardiac or aortic involvement is present, the prognosis can worsen significantly. Pathological assessment often plays a key role in reaching a definite diagnosis of cardiac or aortic vasculitis, particularly when the clinical evidence of a systemic inflammatory disease is missing. The following review will focus on the main histopathological findings of cardiac and aortic vasculitides.
Keywords: aorta; autopsy; cardiovascular pathology; coronary arteries; vasculitis.
Copyright © 2024 Società Italiana di Anatomia Patologica e Citopatologia Diagnostica, Divisione Italiana della International Academy of Pathology.
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Watts RA, Robson J. Introduction, epidemiology and classification of vasculitis. Best Pract Res Clin Rheumatol. 2018;32(1):3-20. https://doi.org/10.1016/j.berh.2018.10.003 10.1016/j.berh.2018.10.003 - DOI - PubMed
-
- Ponte C, Águeda AF, Luqmani RA. Clinical features and structured clinical evaluation of vasculitis. Best Pract Res Clin Rheumatol. 2018;32(1):31-51. https://doi.org/10.1016/j.berh.2018.10.001 10.1016/j.berh.2018.10.001 - DOI - PubMed
-
- Silveira LH. Cardiovascular Manifestations of Systemic Vasculitides. Curr Rheumatol Rep. 2020;22(10):72. https://doi.org/10.1007/s11926-020-00952-1 10.1007/s11926-020-00952-1 - DOI - PubMed
-
- Jennette JC, Falk RJ, Bacon PA, et al. 2012 revised International Chapel Hill Consensus Conference Nomenclature of Vasculitides. Arthritis Rheum. 2013;65(1):1-11. https://doi.org/10.1002/art.37715 10.1002/art.37715 - DOI - PubMed
-
- Domínguez-Quintana M, Alba MA, Hinojosa-Azaola A. Classification of ANCA-associated vasculitis: differences based on ANCA specificity and clinicopathologic phenotype. Rheumatol Int. 2021;41(10):1717-1728. https://doi.org/10.1007/s00296-021-04966-5 10.1007/s00296-021-04966-5 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
