

Effect of Individualized PEEP Guided by Driving Pressure on Diaphragm Function in Patients Undergoing Laparoscopic Radical Resection of Colorectal Cancer: A Randomized Controlled Trial
- PMID: 38768093
- PMCID: PMC11119925
- DOI: 10.12659/MSM.944022
Effect of Individualized PEEP Guided by Driving Pressure on Diaphragm Function in Patients Undergoing Laparoscopic Radical Resection of Colorectal Cancer: A Randomized Controlled Trial
Abstract
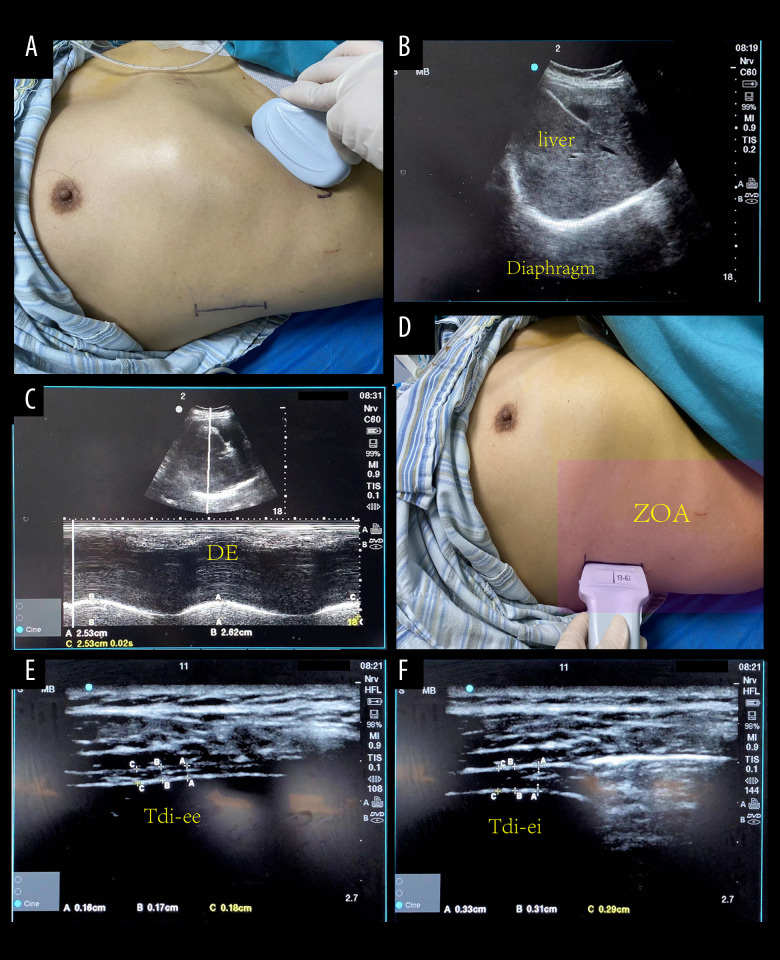
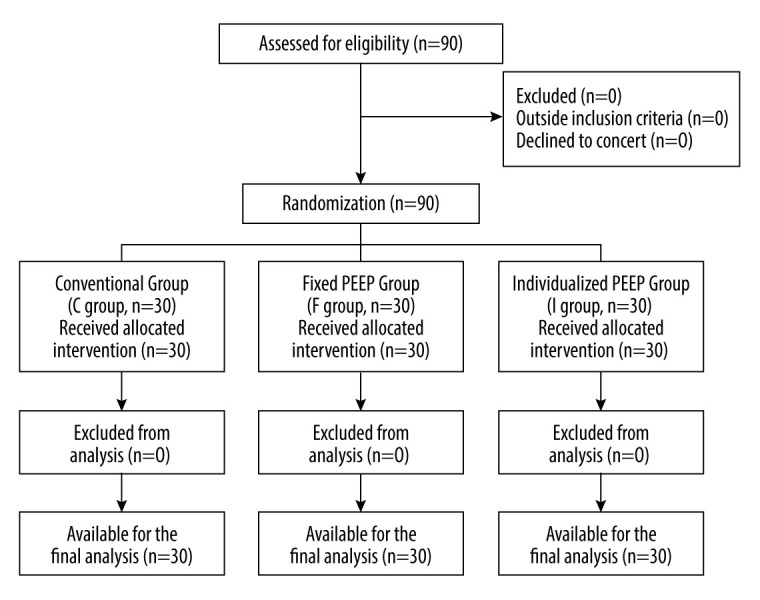
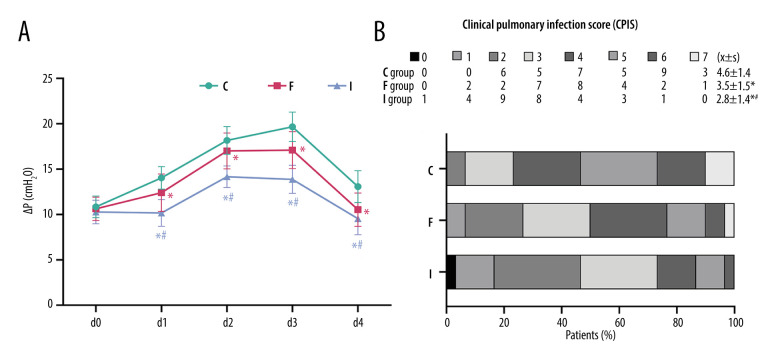
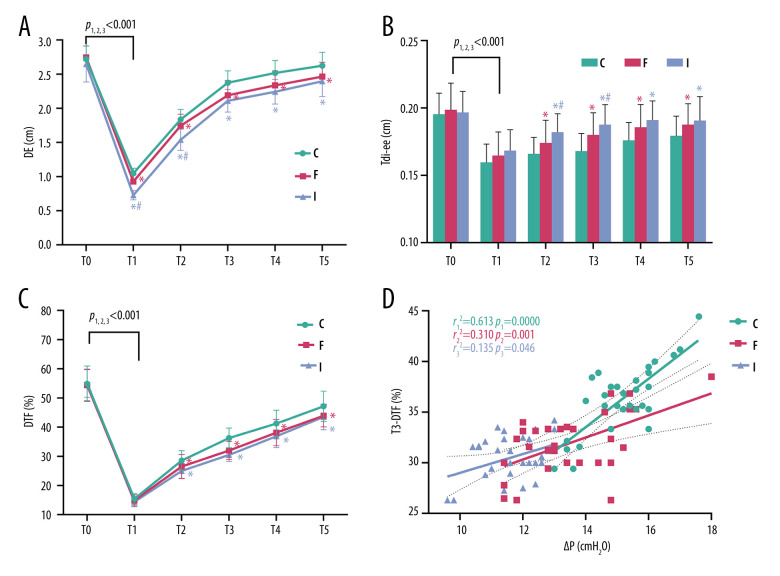
BACKGROUND The concept of driving pressure (ΔP) has been established to optimize mechanical ventilation-induced lung injury. However, little is known about the specific effects of setting individualized positive end-expiratory pressure (PEEP) with driving pressure guidance on patient diaphragm function. MATERIAL AND METHODS Ninety patients were randomized into 3 groups, with PEEP set to 0 in group C; 5 cmH₂O in group F; and individualized PEEP in group I, based on esophageal manometry. Diaphragm ultrasound was performed in the supine position at 6 consecutive time points from T0-T5: diaphragm excursion, end-expiratory diaphragm thickness (Tdi-ee), and diaphragm thickening fraction (DTF) were measured. Primary indicators included diaphragm excursion, Tdi-ee, and DTF at T0-T5, and the correlation between postoperative DTF and ΔP. Secondary indicators included respiratory mechanics, hemodynamic changes at intraoperative d0-d4 time points, and postoperative clinical pulmonary infection scores. RESULTS (1) Diaphragm function parameters reached the lowest point at T1 in all groups (P<0.001). (2) Compared with group C, diaphragm excursion decreased, Tdi-ee increased, and DTF was lower in groups I and F at T1-T5, with significant differences (P<0.05), but the differences between groups I and F were not significant (P>0.05). (3) DTF was significantly and positively correlated with mean intraoperative ΔP in each group at T3, and the correlation was stronger at higher levels of ΔP. CONCLUSIONS Individualized PEEP, achieved by esophageal manometry, minimizes diaphragmatic injury caused by mechanical ventilation based on lung protection, but its protection of the diaphragm during laparoscopic surgery is not superior to that of conventional ventilation strategies.
Conflict of interest statement
Figures
Similar articles
-
Effect of driving pressure-guided individualized positive end-expiratory pressure (PEEP) ventilation strategy on postoperative atelectasis in patients undergoing laparoscopic surgery as assessed by ultrasonography: study protocol for a prospective randomized controlled trial.Trials. 2025 Mar 26;26(1):106. doi: 10.1186/s13063-025-08819-5. Trials. 2025. PMID: 40140868 Free PMC article.
-
Effects of dynamic individualized PEEP guided by driving pressure in laparoscopic surgery on postoperative atelectasis in elderly patients: a prospective randomized controlled trial.BMC Anesthesiol. 2022 Mar 16;22(1):72. doi: 10.1186/s12871-022-01613-9. BMC Anesthesiol. 2022. PMID: 35296253 Free PMC article. Clinical Trial.
-
Effects of driving pressure-guided ventilation by individualized positive end-expiratory pressure on oxygenation undergoing robot-assisted laparoscopic radical prostatectomy: a randomized controlled clinical trial.J Anesth. 2023 Dec;37(6):896-904. doi: 10.1007/s00540-023-03251-y. Epub 2023 Sep 14. J Anesth. 2023. PMID: 37707572 Clinical Trial.
-
Association between driving pressure and development of postoperative pulmonary complications in patients undergoing mechanical ventilation for general anaesthesia: a meta-analysis of individual patient data.Lancet Respir Med. 2016 Apr;4(4):272-80. doi: 10.1016/S2213-2600(16)00057-6. Epub 2016 Mar 4. Lancet Respir Med. 2016. PMID: 26947624 Review.
-
Perioperative Diaphragm Dysfunction.J Clin Med. 2024 Jan 17;13(2):519. doi: 10.3390/jcm13020519. J Clin Med. 2024. PMID: 38256653 Free PMC article. Review.
Cited by
-
Effect of driving pressure-guided positive end-expiratory pressure on respiratory mechanics and clinical outcomes in surgical patients: a systematic review and meta-analysis of randomized controlled trials.Ann Med. 2025 Dec;57(1):2543978. doi: 10.1080/07853890.2025.2543978. Epub 2025 Aug 8. Ann Med. 2025. PMID: 40781750 Free PMC article.
References
-
- Goligher EC, Dres M, Fan E, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. 2018;197(2):204–13. - PubMed
-
- Mocan L. Laparoscopic surgery for the treatment of colon cancer: The new standard? Eur Rev Med Pharmacol Sci. 2021;25(12):4228–35. - PubMed
-
- Oti C, Mahendran M, Sabir N. Anaesthesia for laparoscopic surgery. Br J Hosp Med (Lond) 2016;77(1):24–28. - PubMed
-
- Matamis D, Soilemezi E, Tsagourias M, et al. Sonographic evaluation of the diaphragm in critically ill patients. Technique and clinical applications. Intensive Care Med. 2013;39(5):801–10. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
