

Clinical evaluation and determinants of response to HBI0101 (BCMA CART) therapy in relapsed/refractory multiple myeloma
- PMID: 38768428
- PMCID: PMC11342176
- DOI: 10.1182/bloodadvances.2024012967
Clinical evaluation and determinants of response to HBI0101 (BCMA CART) therapy in relapsed/refractory multiple myeloma
Abstract
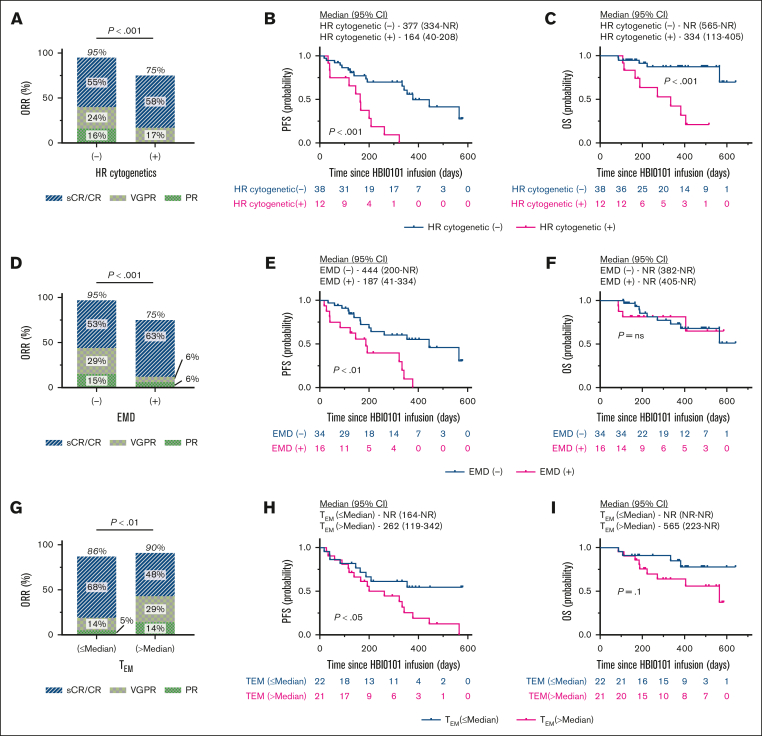
HBI0101 is an academic chimeric antigen receptor T-cell (CART)-targeted to B-cell maturation antigen (BCMA) for the treatment of relapsed and refractory multiple myeloma (R/RMM) and light chain amyloidosis. Herein, we present the phase 1b/2 results of 50 heavily pretreated patients with R/RMM dosed with 800 × 106 CART cells. Inclusion criteria were relatively permissive (i.e., performance status and baseline organ function) and consequently, approximately half of the enrolled patients would have been ineligible for pivotal clinical trials. The median time elapsed from patient enrollment until CART delivery was 25 days (range, 14-65). HBI0101-related toxicities included grade 1 to 3 cytokine release syndrome, grade 3 to 4 hematologic toxicities, and grade 1 to 2 immune effector cell-associated neurotoxicity syndrome. Responses were achieved in 90% of the patients, 56% achieved stringent and complete response, and 70% reached a minimal residual disease negativity. Within a median follow-up of 12.3 months, the median progression-free survival (PFS) was 11.0 months (95% confidence interval [CI], 6.2-14.6), and the overall survival was not reached (95% CI, 13.3 to not reached). Multivariable analysis on patient/disease and CART-related characteristics revealed that high-risk cytogenetic, extramedullary disease, and increased number of effector-memory T cells in CART products were independently associated with inferior PFS. In conclusion, comprehensive analyses of the parameters affecting the response to CART therapy are essential for improving patients' outcome. This trial was registered at www.ClinicalTrials.gov as #NCT04720313.
© 2024 by The American Society of Hematology. Licensed under Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International (CC BY-NC-ND 4.0), permitting only noncommercial, nonderivative use with attribution. All other rights reserved.
Conflict of interest statement
Conflict-of-interest disclosure: S.K.-E., N.A., C.J.C., and P.S. are inventors on patents on the use of anti–B-cell maturation antigen in CART to target multiple myeloma. The remaining authors declare no competing financial interests.
Figures





References
-
- Munshi NC, Anderson LD, Jr., Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
