

Dysregulation of Plasma Growth Factors and Chemokines in Cocaine Use Disorder: Implications for Dual Diagnosis with Schizophrenia and Antisocial Personality Disorder in an Exploratory Study
- PMID: 38768577
- PMCID: PMC11210571
- DOI: 10.1159/000536265
Dysregulation of Plasma Growth Factors and Chemokines in Cocaine Use Disorder: Implications for Dual Diagnosis with Schizophrenia and Antisocial Personality Disorder in an Exploratory Study
Abstract
Introduction: Dual diagnosis in individuals with cocaine use disorders (CUDs) presents a mental health challenge marked by an increased susceptibility to disabling morbidities and premature mortality. Despite extensive research on depression and anxiety, other prevalent comorbidities, such as psychotic and personality disorders, have received less attention. This study explores inflammation-related mediators as potential biomarkers for CUD and dual diagnosis with schizophrenia (SCZ) or antisocial personality disorder (APD).
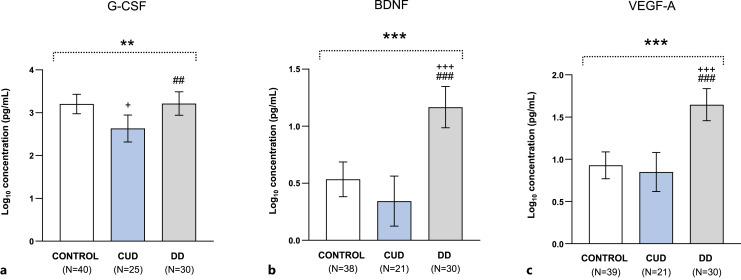
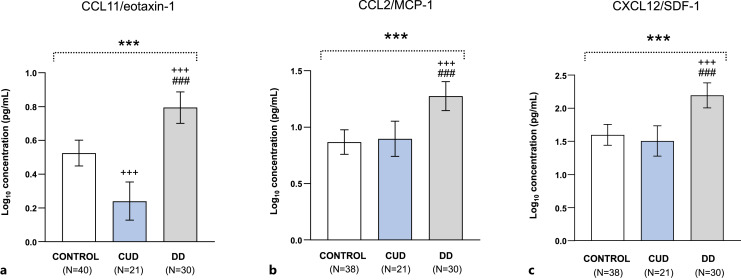
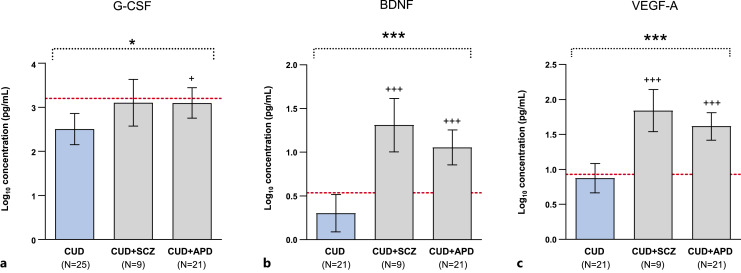
Methods: This exploratory study included 95 participants, comprising 40 healthy subjects and 55 abstinent patients with CUD. Lifetime CUD was diagnosed either as single diagnosis (CUD group, N = 25) or as a dual diagnosis (DD group. N = 30) with SCZ (CUD+SCZ subgroup) or APD (CUD+APD subgroup). Participants were clinically assessed, and the plasma concentrations of growth factors (i.e., G-CSF, BDNF, and VEGF-A) and chemokines (i.e., CCL11/eotaxin-1, CCL2/MCP-1, and CXCL12/SDF-1) were determined and log(10)-transformed for analysis.
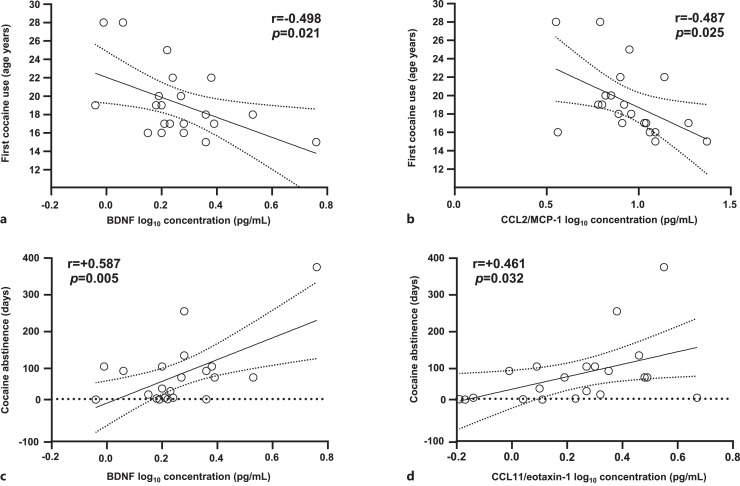
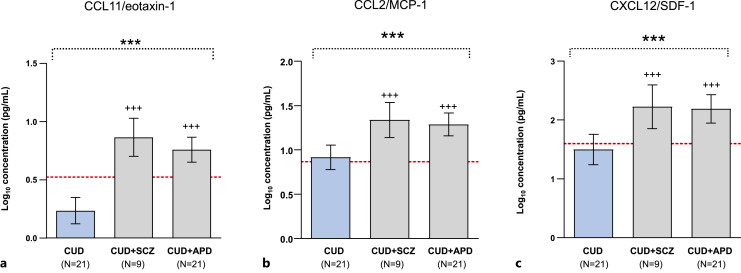
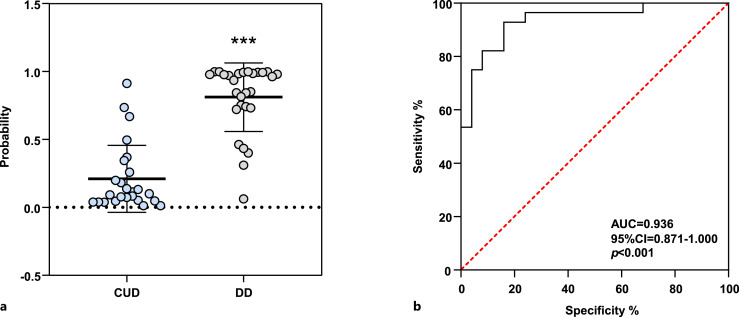
Results: Growth factors and chemokines were dysregulated by CUD and psychiatric diagnoses. Specifically, patients in the CUD group exhibited significantly lower concentrations of G-CSF and CCL11/eotaxin-1 than the control group. In contrast, the DD group showed significantly higher concentrations of all analytes than both the CUD and control groups. Additionally, no differences in these analytes were observed between the CUD+SCZ and CUD+APD subgroups within the DD group. Regarding cocaine-related variables, significant associations were identified in the CUD group: an inverse correlation between the age at first cocaine use and the concentrations of BDNF and CCL2/MCP-1; and a positive correlation between the duration of the cocaine abstinence and the concentrations of BDNF and CCL11/eotaxin-1. Lastly, a logistic regression model incorporating all these analytes demonstrated high discriminatory power in distinguishing patients with CUD alone from those with dual diagnosis.
Conclusions: Individuals with dual diagnosis of CUD exhibit elevated concentrations of growth factors and chemokines, distinguishing them from those with CUD alone. It is unclear whether the differences in these inflammatory mediators are specific to the presence of SCZ and APD. The study highlights potential biomarkers and associations, providing valuable insights into the intricate interplay of CUD and psychiatric disorders to enhance clinical diagnosis and therapeutics.
Keywords: Antisocial personality disorder; BDNF; Chemokines; Cocaine; Dual diagnosis; Eotaxin-1; Growth factors; Schizophrenia.
© 2024 The Author(s). Published by S. Karger AG, Basel.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Figures
References
-
- Herrero MJ, Domingo-Salvany A, Torrens M, Brugal MT; ITINERE Investigators . Psychiatric comorbidity in young cocaine users: induced versus independent disorders. Addiction. 2008;103(2):284–93. - PubMed
-
- Araos P, Vergara-Moragues E, Pedraz M, Pavón FJ, Campos Cloute R, Calado M, et al. Comorbilidad psicopatológica en consumidores de cocaína en tratamiento ambulatorio. Adicciones. 2014;26(1):15–26. - PubMed
-
- Alías-Ferri M, García-Marchena N, Mestre-Pintó JI, Araos P, Vergara-Moragues E, Fonseca F, et al. Cocaine and depressive disorders: when standard clinical diagnosis is insufficient. Adicciones. 2021;33(3):193–200. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
