

Fatal COVID-19 pulmonary disease involves ferroptosis
- PMID: 38769293
- PMCID: PMC11106344
- DOI: 10.1038/s41467-024-48055-0
Fatal COVID-19 pulmonary disease involves ferroptosis
Abstract
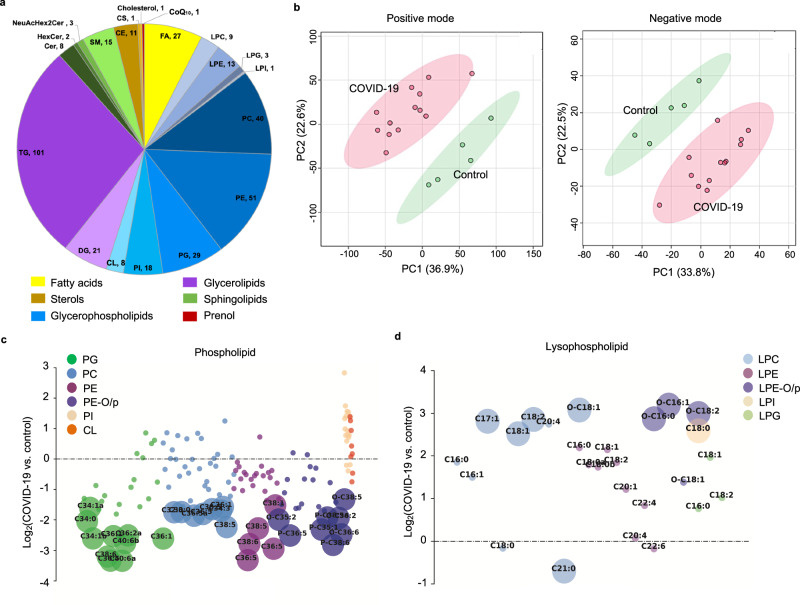
SARS-CoV-2 infection causes severe pulmonary manifestations, with poorly understood mechanisms and limited treatment options. Hyperferritinemia and disrupted lung iron homeostasis in COVID-19 patients imply that ferroptosis, an iron-dependent cell death, may occur. Immunostaining and lipidomic analysis in COVID-19 lung autopsies reveal increases in ferroptosis markers, including transferrin receptor 1 and malondialdehyde accumulation in fatal cases. COVID-19 lungs display dysregulation of lipids involved in metabolism and ferroptosis. We find increased ferritin light chain associated with severe COVID-19 lung pathology. Iron overload promotes ferroptosis in both primary cells and cancerous lung epithelial cells. In addition, ferroptosis markers strongly correlate with lung injury severity in a COVID-19 lung disease model using male Syrian hamsters. These results reveal a role for ferroptosis in COVID-19 pulmonary disease; pharmacological ferroptosis inhibition may serve as an adjuvant therapy to prevent lung damage during SARS-CoV-2 infection.
© 2024. The Author(s).
Conflict of interest statement
B.R.S. is an inventor on patents and patent applications involving ferroptosis; co-founded and serves as a consultant to ProJenX, Inc. and Exarta Therapeutics; holds equity in Sonata Therapeutics; serves as a consultant to Weatherwax Biotechnologies Corporation and Akin Gump Strauss Hauer & Feld LLP. B.R.S. and H.T. are inventors on a patent application related to ferrostatin-1 analog development. B.Q. is now a Post Doc Scientist at Gilead Sciences, Inc. The remaining authors declare no competing interests.
Figures



References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Miscellaneous
