

Mortality and cardiac arrest rates of emergency surgery in developed and developing countries: a systematic review and meta-analysis
- PMID: 38769493
- PMCID: PMC11104000
- DOI: 10.1186/s12871-024-02559-w
Mortality and cardiac arrest rates of emergency surgery in developed and developing countries: a systematic review and meta-analysis
Abstract
Background: The magnitude of the risk of death and cardiac arrest associated with emergency surgery and anesthesia is not well understood. Our aim was to assess whether the risk of perioperative and anesthesia-related death and cardiac arrest has decreased over the years, and whether the rates of decrease are consistent between developed and developing countries.
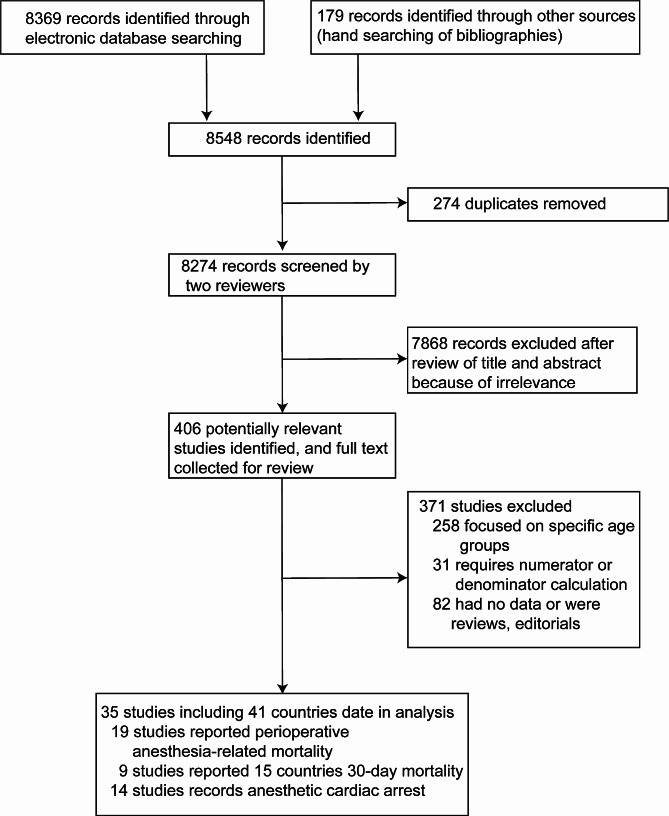
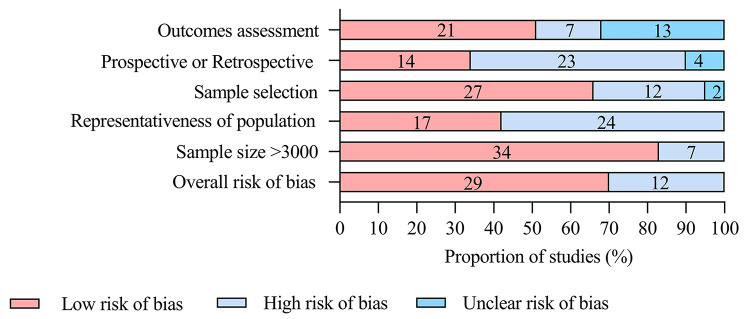
Methods: A systematic review was performed using electronic databases to identify studies in which patients underwent emergency surgery with rates of perioperative mortality, 30-day postoperative mortality, or perioperative cardiac arrest. Meta-regression and proportional meta-analysis with 95% confidence intervals (CIs) were performed to evaluate global data on the above three indicators over time and according to country Human Development Index (HDI), and to compare these results according to country HDI status (low vs. high HDI) and time period (pre-2000s vs. post-2000s).
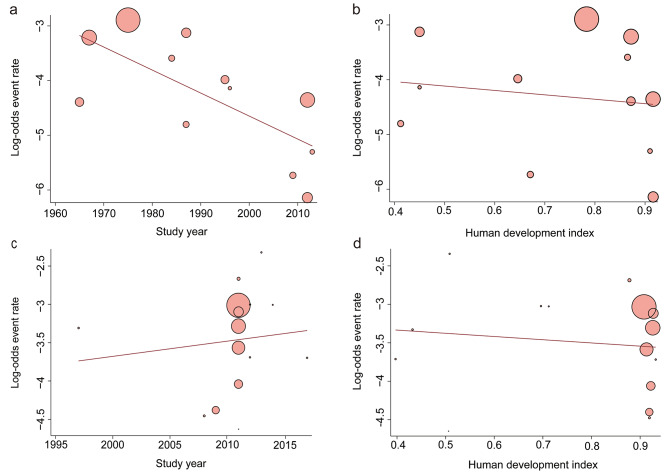
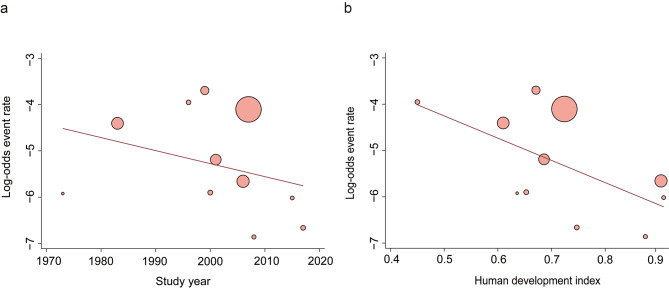
Results: 35 studies met the inclusion criteria, representing more than 3.09 million anesthetic administrations to patients undergoing anesthesia for emergency surgery. Meta-regression showed a significant association between the risk of perioperative mortality and time (slope: -0.0421, 95%CI: from - 0.0685 to -0.0157; P = 0.0018). Perioperative mortality decreased over time from 227 per 10,000 (95% CI 134-380) before the 2000s to 46 (16-132) in the 2000-2020 s (p < 0-0001), but not with increasing HDI. 30-day postoperative mortality did not change significantly (346 [95% CI: 303-395] before the 2000s to 292 [95% CI: 201-423] in the 2000s-2020 period, P = 0.36) and did not decrease with increasing HDI status. Perioperative cardiac arrest rates decreased over time, from 113 per 10,000 (95% CI: 31-409) before the 2000s to 31 (14-70) in the 2000-2020 s, and also with increasing HDI (68 [95% CI: 29-160] in the low-HDI group to 21 [95% CI: 6-76] in the high-HDI group, P = 0.012).
Conclusions: Despite increasing baseline patient risk, perioperative mortality has decreased significantly over the past decades, but 30-day postoperative mortality has not. A global priority should be to increase long-term survival in both developed and developing countries and to reduce overall perioperative cardiac arrest through evidence-based best practice in developing countries.
Keywords: 30-day postoperative mortality; Cardiac arrests; Emergency surgery; Perioperative mortality.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Anesthesia-Related and Perioperative Cardiac Arrest in Low- and High-Income Countries: A Systematic Review With Meta-Regression and Proportional Meta-Analysis.Medicine (Baltimore). 2015 Sep;94(36):e1465. doi: 10.1097/MD.0000000000001465. Medicine (Baltimore). 2015. PMID: 26356701 Free PMC article.
-
Association between intra-operative cardiac arrest and country Human Development Index status: a systematic review with meta-regression analysis and meta-analysis of observational studies.Anaesthesia. 2021 Sep;76(9):1259-1273. doi: 10.1111/anae.15374. Epub 2021 Jan 29. Anaesthesia. 2021. PMID: 33512708
-
Global anaesthesia-related cardiac arrest rates in children: a systematic review and meta-analysis.Br J Anaesth. 2023 Nov;131(5):901-913. doi: 10.1016/j.bja.2023.08.023. Epub 2023 Sep 22. Br J Anaesth. 2023. PMID: 37743151
-
Perioperative mortality in older patients: a systematic review with a meta-regression analysis and meta-analysis of observational studies.J Clin Anesth. 2021 May;69:110160. doi: 10.1016/j.jclinane.2020.110160. Epub 2020 Dec 15. J Clin Anesth. 2021. PMID: 33338975
-
Perioperative and anesthesia-related cardiac arrests in geriatric patients: a systematic review using meta-regression analysis.Sci Rep. 2017 Jun 1;7(1):2622. doi: 10.1038/s41598-017-02745-6. Sci Rep. 2017. PMID: 28572583 Free PMC article.
References
-
- Tamdee D, Charuluxananan S, Punjasawadwong Y, Tawichasri C, Kyokong O, Patumanond J, Rodanant O, Leelanukrom R. Factors related to 24-hour perioperative cardiac arrest in geriatric patients in a Thai university hospital. J Med Assoc Thai. 2009;92(2):198–207. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
