

Identification of neurological complications in childhood influenza: a random forest model
- PMID: 38769496
- PMCID: PMC11103977
- DOI: 10.1186/s12887-024-04773-4
Identification of neurological complications in childhood influenza: a random forest model
Abstract
Background: Among the neurological complications of influenza in children, the most severe is acute necrotizing encephalopathy (ANE), with a high mortality rate and neurological sequelae. ANE is characterized by rapid progression to death within 1-2 days from onset. However, the knowledge about the early diagnosis of ANE is limited, which is often misdiagnosed as simple seizures/convulsions or mild acute influenza-associated encephalopathy (IAE).
Objective: To develop and validate an early prediction model to discriminate the ANE from two common neurological complications, seizures/convulsions and mild IAE in children with influenza.
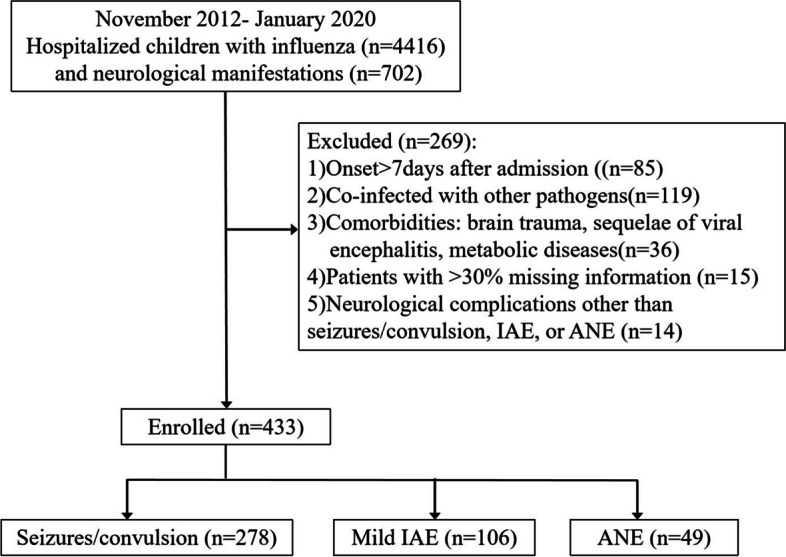
Methods: This retrospective case-control study included patients with ANE (median age 3.8 (2.3,5.4) years), seizures/convulsions alone (median age 2.6 (1.7,4.3) years), or mild IAE (median age 2.8 (1.5,6.1) years) at a tertiary pediatric medical center in China between November 2012 to January 2020. The random forest algorithm was used to screen the characteristics and construct a prediction model.
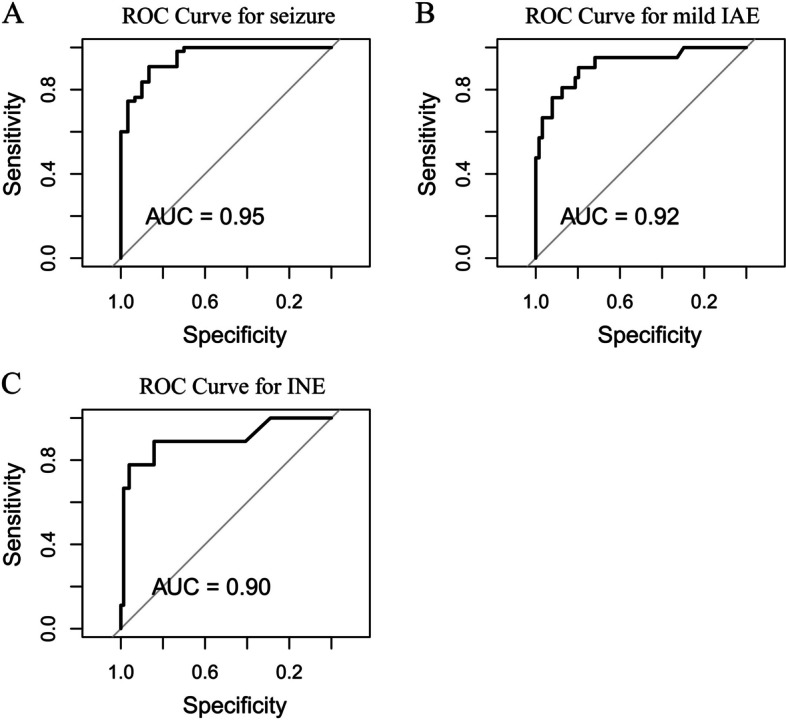
Results: Of the 433 patients, 278 (64.2%) had seizures/convulsions alone, 106 (24.5%) had mild IAE, and 49 (11.3%) had ANE. The discrimination performance of the model was satisfactory, with an accuracy above 0.80 from both model development (84.2%) and internal validation (88.2%). Seizures/convulsions were less likely to be wrongly classified (3.7%, 2/54), but mild IAE (22.7%, 5/22) was prone to be misdiagnosed as seizures/convulsions, and a small proportion (4.5%, 1/22) of them was prone to be misdiagnosed as ANE. Of the children with ANE, 22.2% (2/9) were misdiagnosed as mild IAE, and none were misdiagnosed as seizures/convulsions.
Conclusion: This model can distinguish the ANE from seizures/convulsions with high accuracy and from mild IAE close to 80% accuracy, providing valuable information for the early management of children with influenza.
Keywords: Acute febrile; Acute necrotizing encephalopathy; Children; Complications; Encephalitis; Influenza; Predictive model.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures



References
-
- Chen Q, Li P, Li S, Xiao W, Yang S, Lu H. Brain Complications with Influenza Infection in Children. J Behav Brain Sci. 2020;10(3):129–152. 10.4236/jbbs.2020.103008.
MeSH terms
Grants and funding
- Pre-NSFC-2019-002/Guangzhou Women and Children's Medical Center, Guangzhou Medical University, Guangdong Provincial Clinical Research Center for Child Health, Guangzhou, 510623, China
- Pre-NSFC-2019-002/Guangzhou Women and Children's Medical Center, Guangzhou Medical University, Guangdong Provincial Clinical Research Center for Child Health, Guangzhou, 510623, China
LinkOut - more resources
Full Text Sources
Medical
