

A cross-sectional study of α-synuclein seed amplification assay in Alzheimer's disease neuroimaging initiative: Prevalence and associations with Alzheimer's disease biomarkers and cognitive function
- PMID: 38770829
- PMCID: PMC11350010
- DOI: 10.1002/alz.13858
A cross-sectional study of α-synuclein seed amplification assay in Alzheimer's disease neuroimaging initiative: Prevalence and associations with Alzheimer's disease biomarkers and cognitive function
Abstract
Introduction: Alzheimer's disease (AD) pathology is defined by β-amyloid (Aβ) plaques and neurofibrillary tau, but Lewy bodies (LBs; 𝛼-synuclein aggregates) are a common co-pathology for which effective biomarkers are needed.
Methods: A validated α-synuclein Seed Amplification Assay (SAA) was used on recent cerebrospinal fluid (CSF) samples from 1638 Alzheimer's Disease Neuroimaging Initiative (ADNI) participants, 78 with LB-pathology confirmation at autopsy. We compared SAA outcomes with neuropathology, Aβ and tau biomarkers, risk-factors, genetics, and cognitive trajectories.
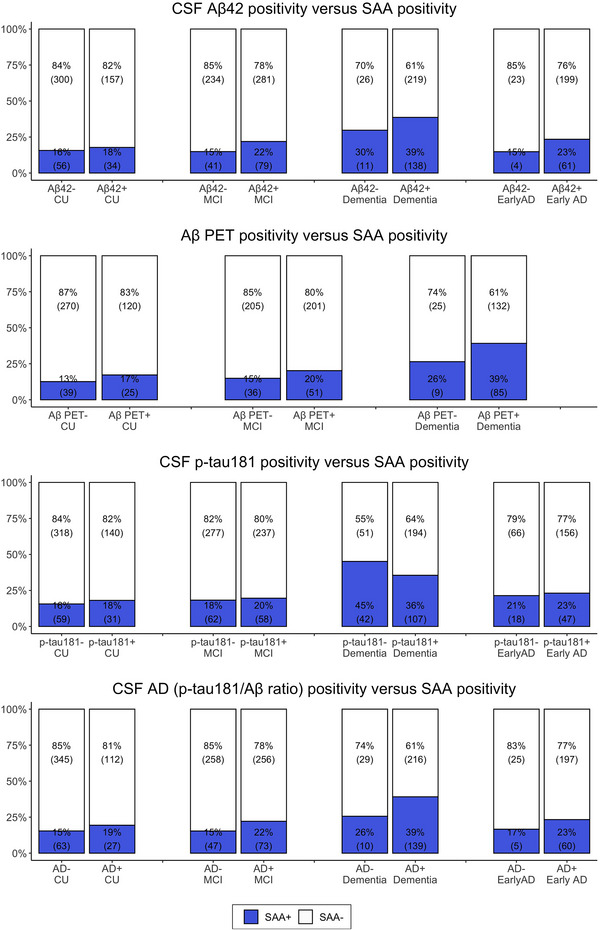
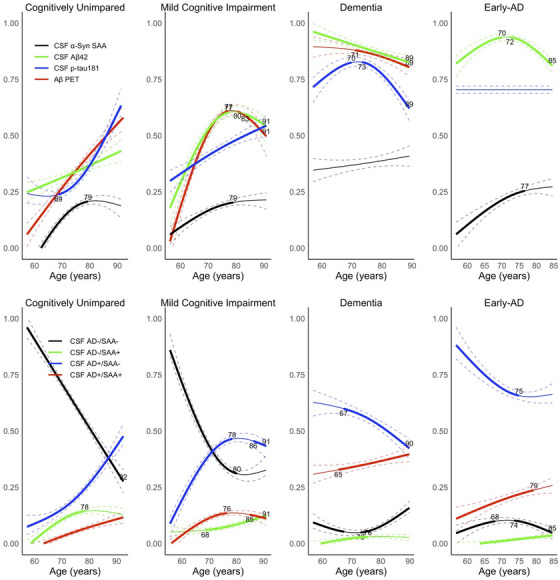
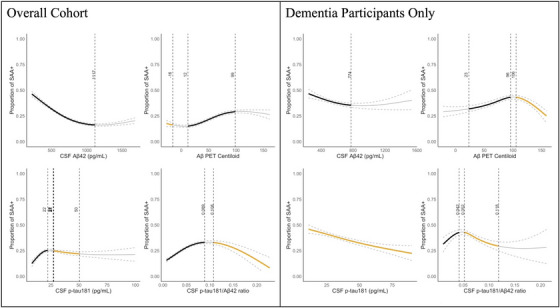
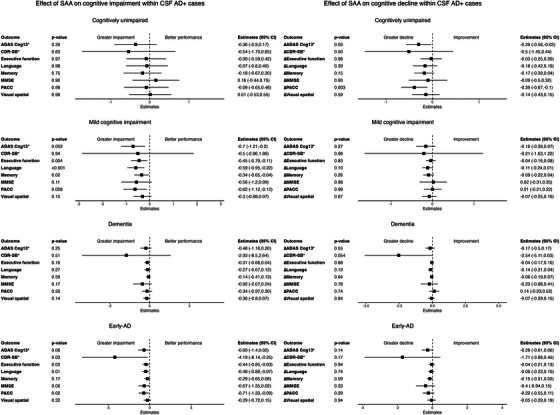
Results: SAA showed 79% sensitivity and 97% specificity for LB pathology, with superior performance in identifying neocortical (100%) compared to limbic (57%) and amygdala-predominant (60%) LB-pathology. SAA+ rate was 22%, increasing with disease stage and age. Higher Aβ burden but lower CSF p-tau181 associated with higher SAA+ rates, especially in dementia. SAA+ affected cognitive impairment in MCI and Early-AD who were already AD biomarker positive.
Discussion: SAA is a sensitive, specific marker for LB-pathology. Its increase in prevalence with age and AD stages, and its association with AD biomarkers, highlights the clinical importance of α-synuclein co-pathology in understanding AD's nature and progression.
Highlights: SAA shows 79% sensitivity, 97% specificity for LB-pathology detection in AD. SAA positivity prevalence increases with disease stage and age. Higher Aβ burden, lower CSF p-tau181 linked with higher SAA+ rates in dementia. SAA+ impacts cognitive impairment in early disease stages. Study underpins need for wider LB-pathology screening in AD treatment.
Keywords: Alzheimer's disease; Lewy body; SAA; co‐pathology.
© 2024 The Authors. Alzheimer's & Dementia published by Wiley Periodicals LLC on behalf of Alzheimer's Association.
Conflict of interest statement
D.T., Z.H., E.B.L., R.J.P, A.J.S., L.M.S., and P.T. receive funding from NIH/NIA. M.A.N. carries out as part of contract work for NIH consultancy. C.B. have nothing to disclose. H.I. is employee of Data Tecnica International and receives NIH support for open science research. J.L., K.M., S.ME., and R.L. are full‐time employee of Amprion Inc and hold stock or stock options of Aprion Inc. A.B.S. receives funding from Intramural Research Program of the National Institutes of Health; received honoraria from Movement Disorders Journal and npjParkinson's Disease; received travel support from Chan Zuckerberg Initiative, Michael J Fox Foundation, and Weill Cornell. M.W.W. serves on Editorial Boards for Alzheimer's & Dementia, and the Journal for Prevention of Alzheimer's disease. He has served on Advisory Boards for Acumen Pharmaceutical, Alzheon, Inc., Cerecin, Merck Sharp & Dohme Corp., and NC Registry for Brain Health. He also serves on the USC ACTC grant which receives funding from Eisai for the AHEAD study. He has provided consulting to BioClinica, Boxer Capital, LLC, Cerecin, Inc., Clario, Dementia Society of Japan, Eisai, Guidepoint, Health and Wellness Partners, Indiana University, LCN Consulting, Merck Sharp & Dohme Corp., NC Registry for Brain Health, Prova Education, T3D Therapeutics, University of Southern California (USC), and WebMD. He has acted as a speaker/lecturer for China Association for Alzheimer's Disease (CAAD) and Taipei Medical University, as well as a speaker/lecturer with academic travel funding provided by: AD/PD Congress, Cleveland Clinic, CTAD Congress, Foundation of Learning; Health Society (Japan), INSPIRE Project; U. Toulouse, Japan Society for Dementia Research, and Korean Dementia Society, Merck Sharp & Dohme Corp., National Center for Geriatrics and Gerontology (NCGG; Japan), University of Southern California (USC). He holds stock options with Alzeca, Alzheon, Inc., ALZPath, Inc., and Anven. Dr Weiner received support for his research from the following funding sources: National Institutes of Health (NIH)/NINDS/National Institute on Aging (NIA), Department of Defense (DOD), California Department of Public Health (CDPH), University of Michigan, Siemens, Biogen, Hillblom Foundation, Alzheimer's Association, Johnson & Johnson, Kevin and Connie Shanahan, GE, VUmc, Australian Catholic University (HBI‐BHR), The Stroke Foundation, and the Veterans Administration. Author disclosures are available in the supporting information.
Figures
References
-
- Kovacs GG, Milenkovic I, Wöhrer A, et al. Non‐Alzheimer neurodegenerative pathologies and their combinations are more frequent than commonly believed in the elderly brain: a community‐based autopsy series. Acta Neuropathol. 2013;126:365‐384. PMID: 23900711. - PubMed
