

Group Multimodal Prenatal Care and Postpartum Outcomes
- PMID: 38771574
- PMCID: PMC11109777
- DOI: 10.1001/jamanetworkopen.2024.12280
Group Multimodal Prenatal Care and Postpartum Outcomes
Abstract
Importance: An increasing body of evidence suggests equivalent if not improved postpartum outcomes of in-person group prenatal care compared with individual prenatal care. However, research is needed to evaluate outcomes of group multimodal prenatal care (GMPC), with groups delivered virtually in combination with individual in-person office appointments to collect vital signs and conduct other tests compared with individual multimodal prenatal care (IMPC) delivered through a combination of remotely delivered and in-person visits.
Objective: To compare postpartum outcomes between GMPC and IMPC.
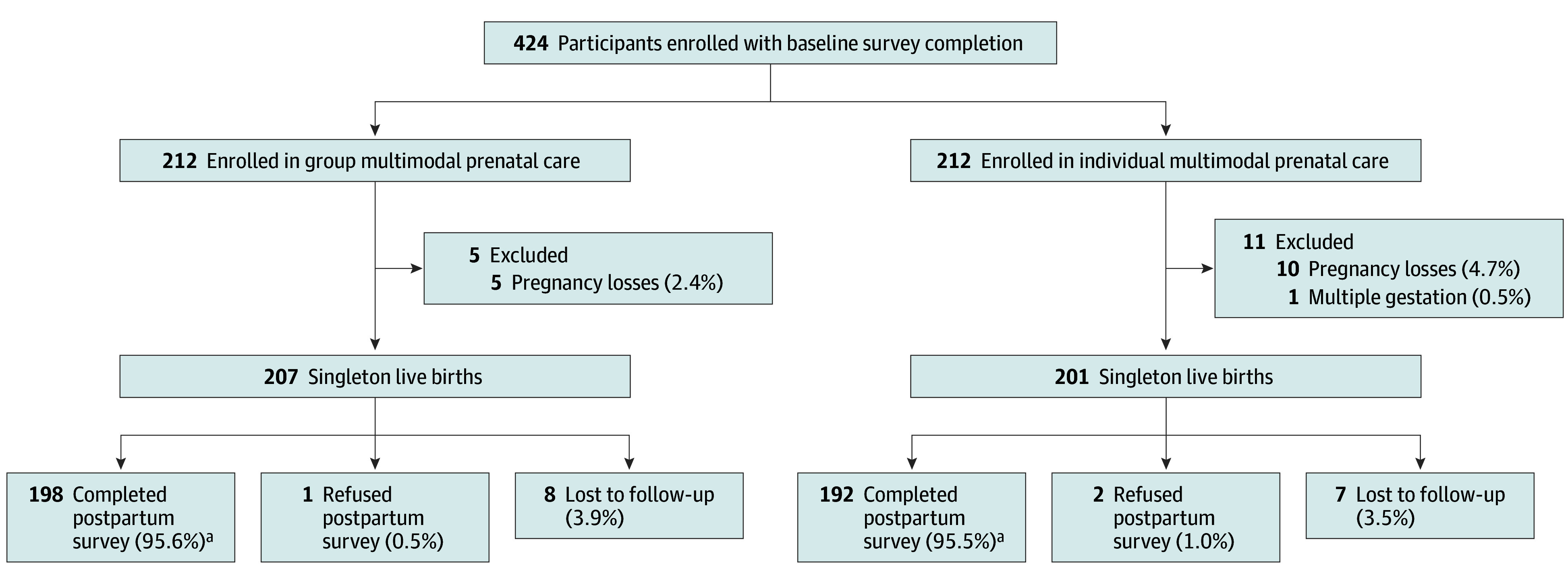
Design, setting, and participants: A frequency-matched longitudinal cohort study was conducted at Kaiser Permanente Northern California, an integrated health care delivery system. Participants included 424 individuals who were pregnant (212 GMPC and 212 frequency-matched IMPC controls (matched on gestational age, race and ethnicity, insurance status, and maternal age) receiving prenatal care between August 17, 2020, and April 1, 2021. Participants completed a baseline survey before 14 weeks' gestation and a follow-up survey between 4 and 8 weeks post partum. Data analysis was performed from January 3, 2022, to March 4, 2024.
Exposure: GMPC vs IMPC.
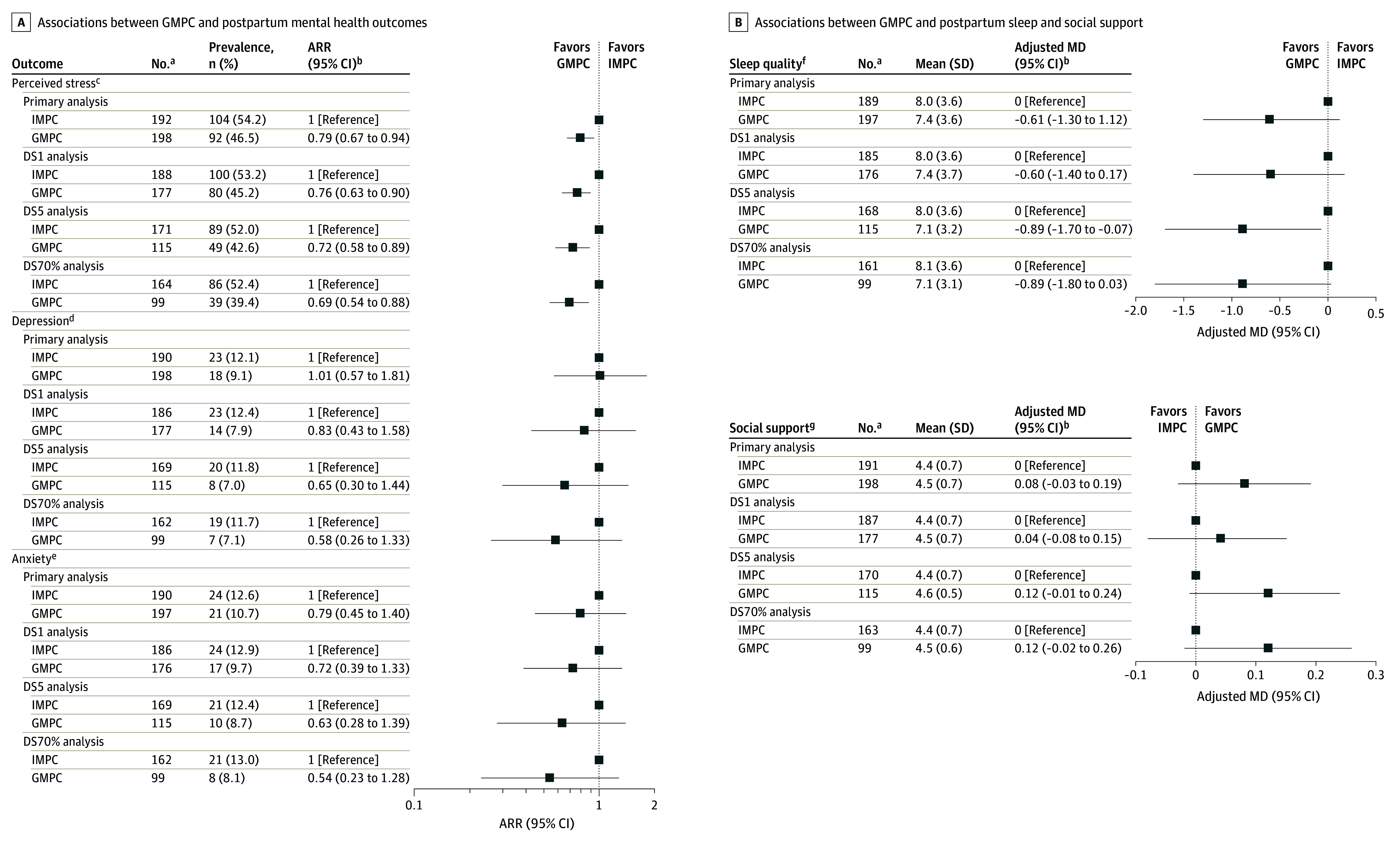
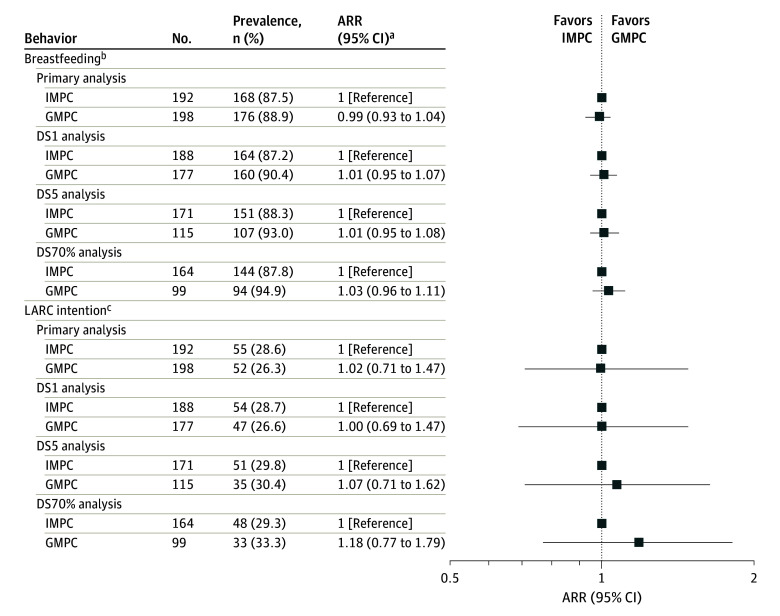
Main outcome measures: Validated instruments were used to ascertain postpartum psychosocial outcomes (stress, depression, anxiety) and perceived quality of prenatal care. Self-reported outcomes included behavioral outcomes (breastfeeding initiation, use of long-acting reversible contraception), satisfaction with prenatal care, and preparation for self and baby care after delivery. Primary analyses included all study participants in the final cohort. Three secondary dose-stratified analyses included individuals who attended at least 1 visit, 5 visits, and 70% of visits. Log-binomial regression and linear regression analyses were conducted.
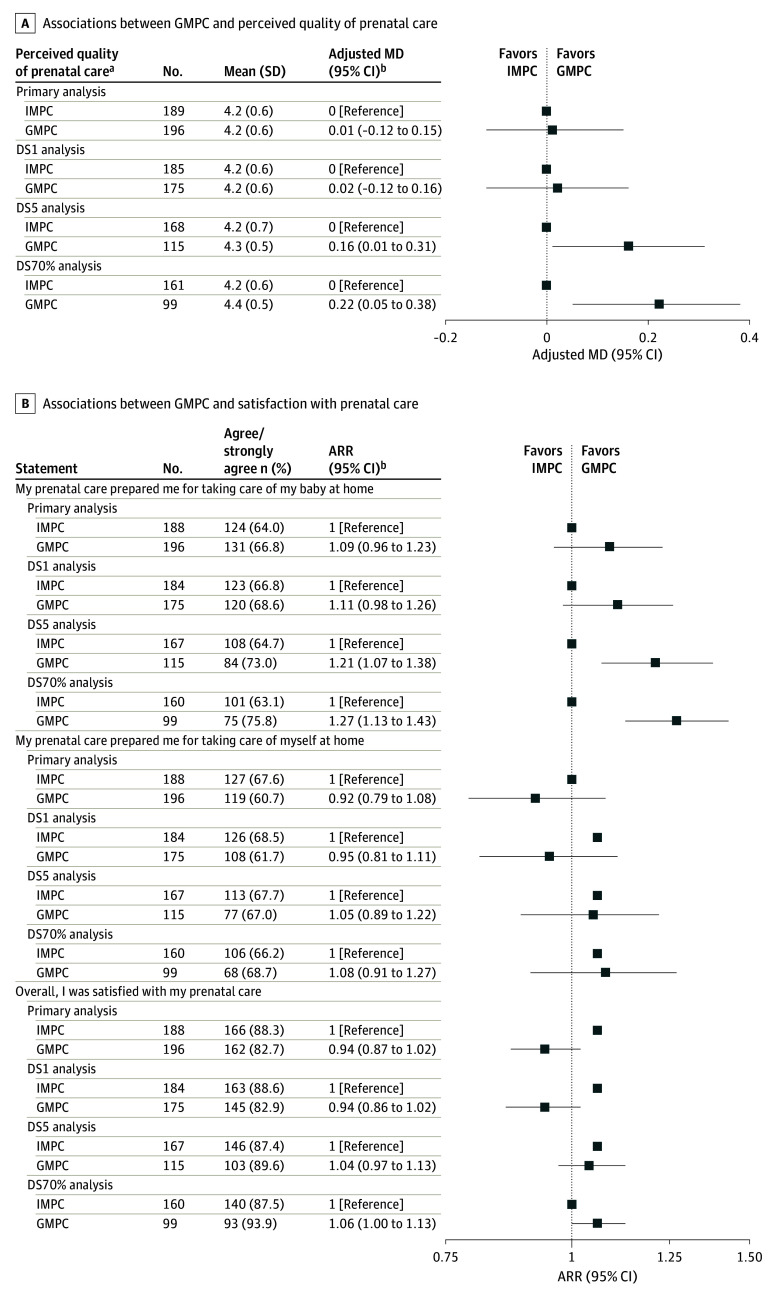
Results: The final analytic cohort of 390 participants (95.6% follow-up rate of 408 singleton live births) was racially and ethnically diverse: 98 (25.1%) Asian/Pacific Islander, 88 (22.6%) Hispanic, 17 (4.4%) non-Hispanic Black, 161 (41.3%) non-Hispanic White, and 26 (6.7%) multiracial participants; median age was 32 (IQR, 30-35) years. In the primary analysis, after adjustment, GMPC was associated with a 21% decreased risk of perceived stress (adjusted risk ratio [ARR], 0.79; 95% CI, 0.67-0.94) compared with IMPC. Findings were consistent in the dose-stratified analyses. There were no significant differences between GMPC and IMPC for other psychosocial outcomes. While in the primary analyses there was no significant group differences in perceived quality of prenatal care (mean difference [MD], 0.01; 95% CI, -0.12 to 0.15) and feeling prepared to take care of baby at home (ARR, 1.09; 95% CI, 0.96-1.23), the dose-stratified analyses documented higher perceived quality of prenatal care (MD, 0.16; 95% CI, 0.01-0.31) and preparation for taking care of baby at home (ARR, 1.27; 95% CI, 1.13-1.43) for GMPC among those attending 70% of visits. No significant differences were noted in patient overall satisfaction with prenatal care and feeling prepared for taking care of themselves after delivery.
Conclusions: In this cohort study, equivalent and, in some cases, better outcomes were observed for GMPC compared with IMPC. Health care systems implementing multimodal models of care may consider incorporating virtual group prenatal care as a prenatal care option for patients.
Conflict of interest statement
Figures
Similar articles
-
Prenatal Health Care Outcomes Before and During the COVID-19 Pandemic Among Pregnant Individuals and Their Newborns in an Integrated US Health System.JAMA Netw Open. 2023 Jul 3;6(7):e2324011. doi: 10.1001/jamanetworkopen.2023.24011. JAMA Netw Open. 2023. PMID: 37462973 Free PMC article.
-
Association of Expanded Prenatal Care Coverage for Immigrant Women With Postpartum Contraception and Short Interpregnancy Interval Births.JAMA Netw Open. 2021 Aug 2;4(8):e2118912. doi: 10.1001/jamanetworkopen.2021.18912. JAMA Netw Open. 2021. PMID: 34338791 Free PMC article.
-
Neighborhood Disadvantage, Race and Ethnicity, and Postpartum Depression.JAMA Netw Open. 2023 Nov 1;6(11):e2342398. doi: 10.1001/jamanetworkopen.2023.42398. JAMA Netw Open. 2023. PMID: 37955900 Free PMC article.
-
Schedules for home visits in the early postpartum period.Cochrane Database Syst Rev. 2021 Jul 21;7(7):CD009326. doi: 10.1002/14651858.CD009326.pub4. Cochrane Database Syst Rev. 2021. PMID: 34286512 Free PMC article.
-
Behavioural modification interventions for medically unexplained symptoms in primary care: systematic reviews and economic evaluation.Health Technol Assess. 2020 Sep;24(46):1-490. doi: 10.3310/hta24460. Health Technol Assess. 2020. PMID: 32975190 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
