

Understanding experiences, unmet needs and priorities related to post-stroke aphasia care: stage one of an experience-based co-design project
- PMID: 38772583
- PMCID: PMC11110611
- DOI: 10.1136/bmjopen-2023-081680
Understanding experiences, unmet needs and priorities related to post-stroke aphasia care: stage one of an experience-based co-design project
Abstract
Objective: People with post-stroke aphasia (language/communication impairment) and their supporters report mixed satisfaction with stroke and aphasia care. To date, however, their journey of care and the key service interactions that shape their experience have not been comprehensively explored. We aimed to investigate the lived experience of post-stroke aphasia care, across the continuum of care and by geographical location, to establish priorities for service design.
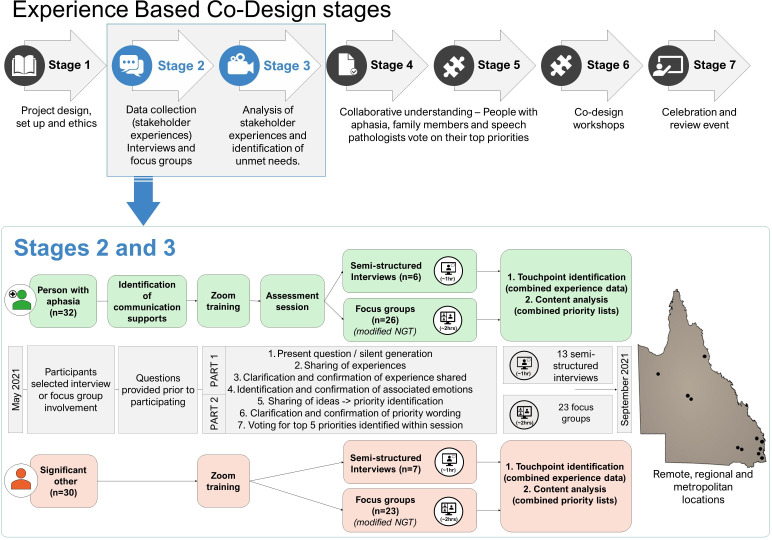
Design: This is the first stage of an experience-based co-design study. We purposively sampled people with aphasia (PWA) and significant others (SOs) across 21 hospital and health service sites, community groups and by self-referral. Participants shared experiences of care in online interviews and focus groups. Touchpoints (key moments that shape experience) and unmet needs were identified using qualitative thematic analysis. Priorities for service design were established using an adapted nominal group technique.
Setting: Sites spanned remote, regional and metropolitan areas in Queensland, Australia.
Participants: PWA (n=32; mild=56%; moderate=31%; severe=13%) and SOs (n=30) shared 124 experiences of acute, rehabilitation and community-based care in 23 focus groups and 13 interviews.
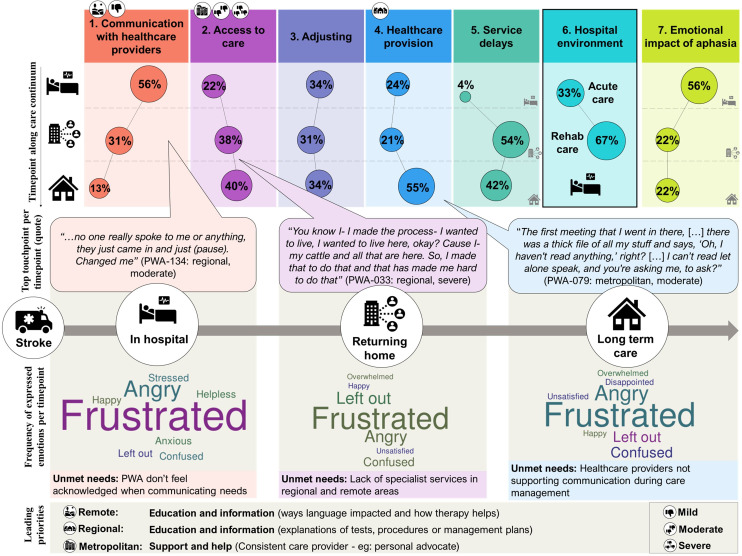
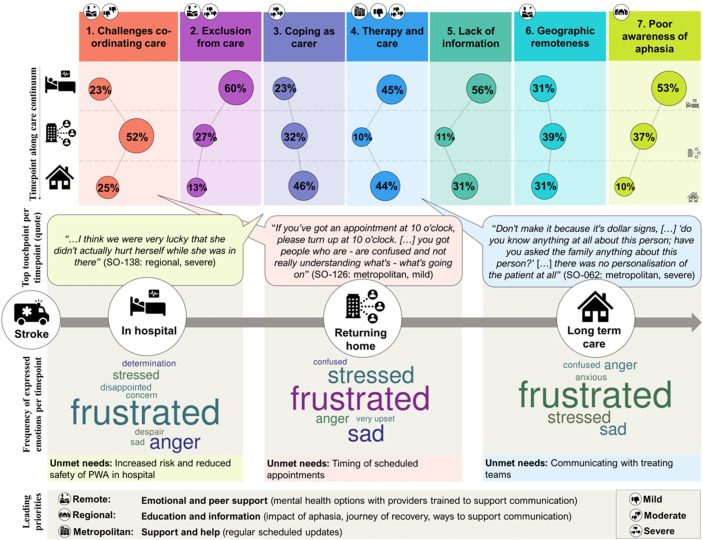
Results: Both positive and negative healthcare experiences occurred most frequently in hospital settings. Negative experiences regularly related to communication with health professionals, while positive experiences related to the interpersonal qualities of healthcare providers (eg, providing hope) for PWA, or witnessing good rapport between a PWA and their health professional for SOs. To improve services, PWA prioritised communicatively accessible education and information and SOs prioritised access to psychological and peer support.
Conclusions: We identified key aspects of post-stroke aphasia care that shape experience. The needs of PWA and SOs may be better met through health professional training in supported communication, increased service availability in regional and remote areas, communication-accessible hospital environments, increased access to psychological and peer support, and meaningful involvement of SOs in rehabilitation.
Keywords: Health Services; Patient-Centered Care; QUALITATIVE RESEARCH; STROKE MEDICINE.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- Mitchell C, Gittins M, Tyson S, et al. Prevalence of aphasia and dysarthria among inpatient stroke survivors: describing the population, therapy provision and outcomes on discharge. Aphasiology 2021;35:950–60. 10.1080/02687038.2020.1759772 - DOI
-
- Stroke Foundation . National stroke audit – acute services report 2015. Melbourne, Australia: 1-38;2015.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous