

Untangling the relationship between smoking and systemic sclerosis: an analysis of the EUSTAR cohort
- PMID: 38772679
- PMCID: PMC11328649
- DOI: 10.1136/rmdopen-2024-004101
Untangling the relationship between smoking and systemic sclerosis: an analysis of the EUSTAR cohort
Abstract
Objectives: To untangle the association between smoking and systemic sclerosis (SSc).
Methods: In the European Scleroderma Trials and Research cohort, the autoantibody status was compared between ever-smokers and never-smokers. Time until disease progression was assessed using Kaplan-Meier curves. Cox models were built to investigate the influence of smoking over 15 years of follow-up. All analyses were performed for the total cohort and stratified for sex and for positivity of anti-centromere (ACA) and anti-topoisomerase antibodies (ATA).
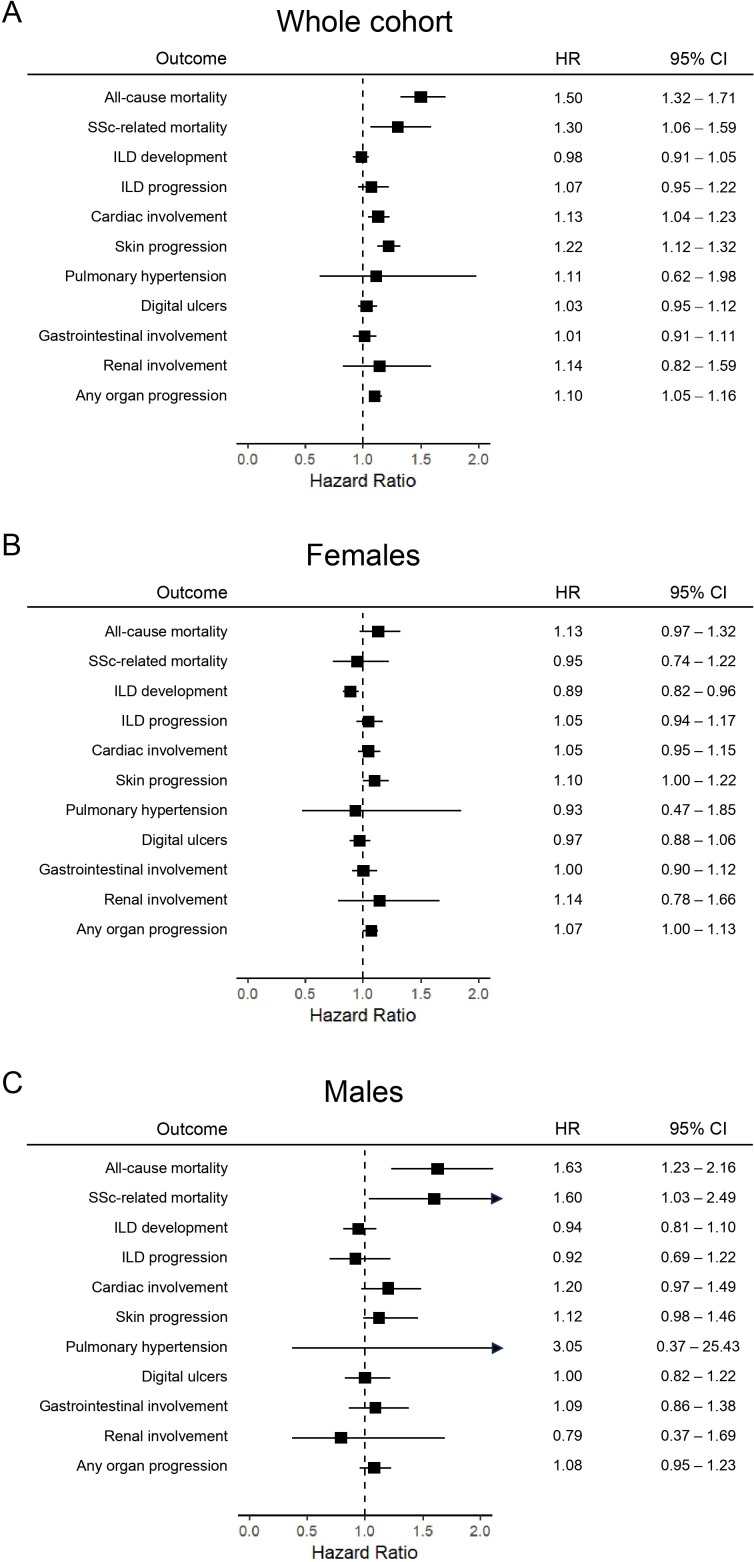
Results: Overall, 12 314 patients were included in the study. Of these, 10 393 were women (84%), 4637 were ACA-positive (38%), 3919 were ATA-positive (32%) and 4271 (35%) were ever-smokers. In men, but not in women, smoking was associated with mortality (HR 1.63, 95% CI 1.23 to 2.16, p=0.001). Ever-smoking women were at higher risk for skin progression (HR 1.10, 95% CI 1.00 to 1.22, p=0.046) and for 'any organ progression' (HR 1.07, 95% CI 1.00 to 1.13, p=0.036). In women, 34% of never-smokers were ATA-positive compared with 21% of ever-smokers (p<0.001). In the group of ever-smokers, higher exposure rates, reflected by the number of pack-years (OR 0.98, 95% CI 0.97 to 0.99, p<0.001) and by smoking duration (OR 0.96, 95% CI 0.95 to 0.97, p<0.001), were associated with lower frequency of ATA. In ACA-positive patients, the risk of mortality (HR 1.29, 95% CI 1.02 to 1.63, p=0.033), cardiac involvement (HR 1.25, 95% CI 1.03 to 1.43, p=0.001), skin progression (HR 1.21, 95% CI 1.03 to 1.42, p=0.018) and 'any organ progression' (HR 1.14, 95% CI 1.05 to 1.24, p=0.002) was increased among smokers. In ATA-positive smoking patients, mortality (HR 1.40, 95% CI 1.10 to 1.78, p=0.006), skin progression (HR 1.19, 95% CI 1.03 to 1.37, p=0.020) digital ulcers (HR 1.17, 95% CI 1.02 to 1.34, p=0.029) and 'any organ progression' (HR 1.11, 95% CI 1.00 to 1.22, p=0.048) occurred more frequently.
Conclusions: Our stratified analysis demonstrates that smoking is associated with an increased risk for mortality in male SSc patients but not in women. Strikingly, smoking is associated with lower prevalence of ATA positivity, in particular in women. In both ATA-positive and ACA-positive patients, smoking is a risk factor for mortality, skin progression and 'any organ progression'.
Keywords: Autoantibodies; Risk Factors; Smoking; Systemic Sclerosis.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures





Similar articles
-
Sex-specific risk of anti-topoisomerase antibodies on mortality and disease severity in systemic sclerosis: 10-year analysis of the Leiden CCISS and EUSTAR cohorts.Lancet Rheumatol. 2022 Oct;4(10):e699-e709. doi: 10.1016/S2665-9913(22)00224-7. Lancet Rheumatol. 2022. PMID: 38265968
-
Smoking and systemic sclerosis: influence on microangiopathy and expression of anti-topoisomerase I antibodies in a monocentric cohort.Clin Exp Rheumatol. 2020 May-Jun;38 Suppl 125(3):25-28. Epub 2020 Mar 25. Clin Exp Rheumatol. 2020. PMID: 32242801
-
Clinical significance of coexisting antitopoisomerase I and anticentromere antibodies in patients with systemic sclerosis: a EUSTAR group-based study.Clin Exp Rheumatol. 2013 Mar-Apr;31(2 Suppl 76):96-102. Epub 2012 Oct 24. Clin Exp Rheumatol. 2013. PMID: 23101460
-
Systemic sclerosis in mother and daughter with susceptible HLA haplotype and anti-topoisomerase I autoantibodies.Rheumatol Int. 2020 Jun;40(6):1001-1009. doi: 10.1007/s00296-020-04516-5. Epub 2020 Jan 22. Rheumatol Int. 2020. PMID: 31970496 Review.
-
Coexistence of antitopoisomerase I and anticentromere antibodies in patients with systemic sclerosis.Ann Rheum Dis. 2002 Feb;61(2):121-7. doi: 10.1136/ard.61.2.121. Ann Rheum Dis. 2002. PMID: 11796397 Free PMC article. Review.
Cited by
-
Sex Bias in Systemic Sclerosis: from Clinical to Immunological Differences.Clin Rev Allergy Immunol. 2025 May 27;68(1):51. doi: 10.1007/s12016-025-09062-1. Clin Rev Allergy Immunol. 2025. PMID: 40423726 Free PMC article. Review.
-
Screening for autoimmune diseases in apparently healthy antinuclear antibody positive individuals.Front Med (Lausanne). 2024 Aug 20;11:1455673. doi: 10.3389/fmed.2024.1455673. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39228805 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials