

Integrative multi-region molecular profiling of primary prostate cancer in men with synchronous lymph node metastasis
- PMID: 38773085
- PMCID: PMC11109137
- DOI: 10.1038/s41467-024-48629-y
Integrative multi-region molecular profiling of primary prostate cancer in men with synchronous lymph node metastasis
Abstract
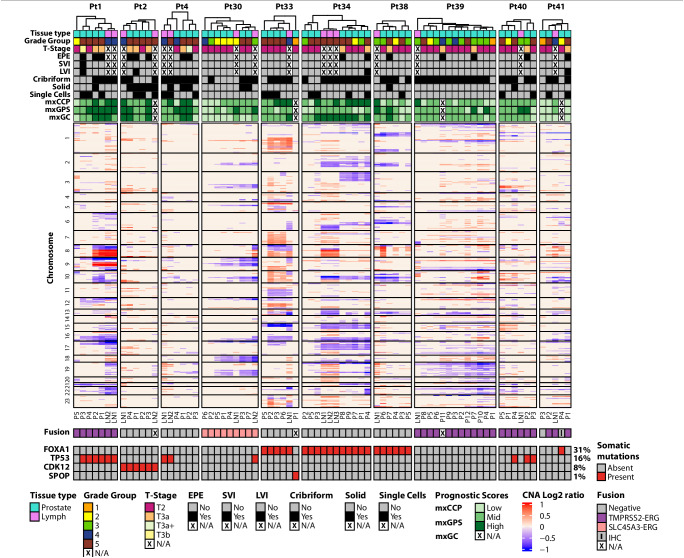
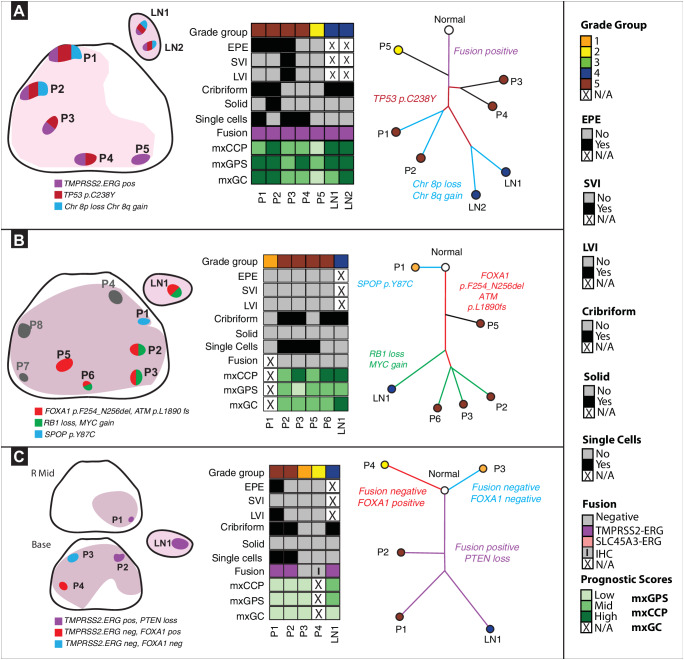
Localized prostate cancer is frequently composed of multiple spatially distinct tumors with significant inter- and intra-tumoral molecular heterogeneity. This genomic diversity gives rise to many competing clones that may drive the biological trajectory of the disease. Previous large-scale sequencing efforts have focused on the evolutionary process in metastatic prostate cancer, revealing a potential clonal progression to castration resistance. However, the clonal origin of synchronous lymph node (LN) metastases in primary disease is still unknown. Here, we perform multi-region, targeted next generation sequencing and construct phylogenetic trees in men with prostate cancer with synchronous LN metastasis to better define the pathologic and molecular features of primary disease most likely to spread to the LNs. Collectively, we demonstrate that a combination of histopathologic and molecular factors, including tumor grade, presence of extra-prostatic extension, cellular morphology, and oncogenic genomic alterations are associated with synchronous LN metastasis.
© 2024. The Author(s).
Conflict of interest statement
The content is solely the responsibility of the authors and does not necessarily represent the official views of U-M Precision Health. JJT is a co-founder with minor equity interest in LynxDx, which has licensed urinary biomarkers unrelated to this project. S.A.T has received travel support from and had a sponsored research agreement with Compendia Bioscience/Life Technologies/ThermoFisher. The University of Michigan and Brigham and Women’s Hospital have been issued a patent on
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
