

Managing failed vital pulp therapies in mature permanent teeth in a retrospective cohort study, with success and survival rates of managing protocols
- PMID: 38773252
- PMCID: PMC11109120
- DOI: 10.1038/s41598-024-62565-3
Managing failed vital pulp therapies in mature permanent teeth in a retrospective cohort study, with success and survival rates of managing protocols
Abstract
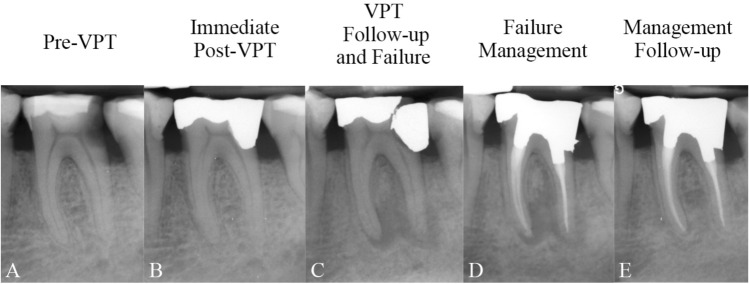
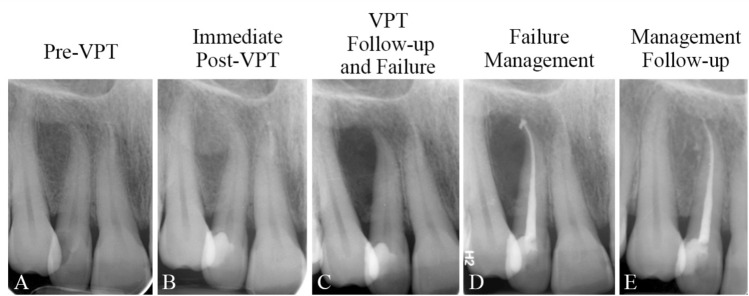
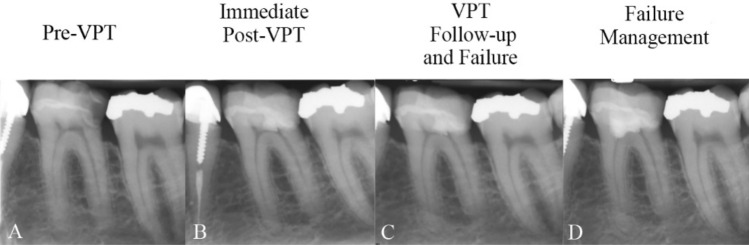
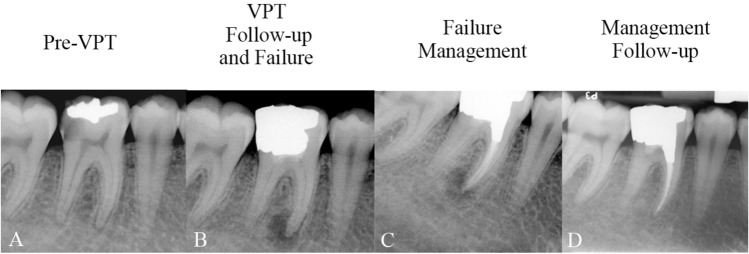
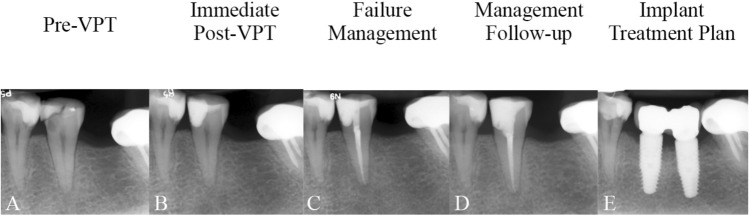
Despite advancements in vital pulp therapy (VPT), a subset of cases fails to achieve desired outcomes. This study based on a previous large-scale cohort study involving 1257 VPT-treated teeth, aiming to describe the demographic data and clinical characteristics of all failed cases and their management protocols. Clinical records/images of 105 failed cases treated by a single endodontist (2011-2022) were examined, including 10 extracted teeth. Asymptomatic cases with PDL widening received no intervention, while others underwent management protocols, including (selective) RCT and (tampon) re-VPT. These retreatments were assessed for success (defined as radiographic evidence of healing) and survival (characterized by the retention/function of the treated tooth) using Kaplan-Meier analysis. While 51.4% of all initial failures were diagnosed due to symptoms, 48.6% were symptom-free. Notably, failed cases with symptomatic irreversible pulpitis, and apical periodontitis/widened PDL before initial treatment significantly outnumbered asymptomatic cases and normal PDL, respectively (P = 0.001). Moreover, most of the initial failures were observed in teeth with composite resin rather than amalgam restorations (P = 0.002). The success and survival rates for the management protocols were 91.78% and 95.79%, respectively, over an average follow-up period of 36.94 (± 23.30) months. RCT and re-VPT procedures provide successful outcomes for managing unsuccessful VPTs.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no conflicts of interest regarding the publication of this paper. Prof. Saeed Asgary is the inventor of CEM cement (Endodontic Filling Material; USA, 7,942,961, 2011 May 17).
Figures



References
-
- Kielbassa AM, Muller J, Gernhardt CR. Closing the gap between oral hygiene and minimally invasive dentistry: A review on the resin infiltration technique of incipient (proximal) enamel lesions. Quintessence Int. 2009;40:663–681. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
