

High-precision stereotactic irradiation for focal drug-resistant epilepsy versus standard treatment: a randomized waitlist-controlled trial (the PRECISION trial)
- PMID: 38773643
- PMCID: PMC11106873
- DOI: 10.1186/s13063-024-08168-9
High-precision stereotactic irradiation for focal drug-resistant epilepsy versus standard treatment: a randomized waitlist-controlled trial (the PRECISION trial)
Abstract
Introduction: The standard treatment for patients with focal drug-resistant epilepsy (DRE) who are not eligible for open brain surgery is the continuation of anti-seizure medication (ASM) and neuromodulation. This treatment does not cure epilepsy but only decreases severity. The PRECISION trial offers a non-invasive, possibly curative intervention for these patients, which consist of a single stereotactic radiotherapy (SRT) treatment. Previous studies have shown promising results of SRT in this patient population. Nevertheless, this intervention is not yet available and reimbursed in the Netherlands. We hypothesize that: SRT is a superior treatment option compared to palliative standard of care, for patients with focal DRE, not eligible for open surgery, resulting in a higher reduction of seizure frequency (with 50% of the patients reaching a 75% seizure frequency reduction at 2 years follow-up).
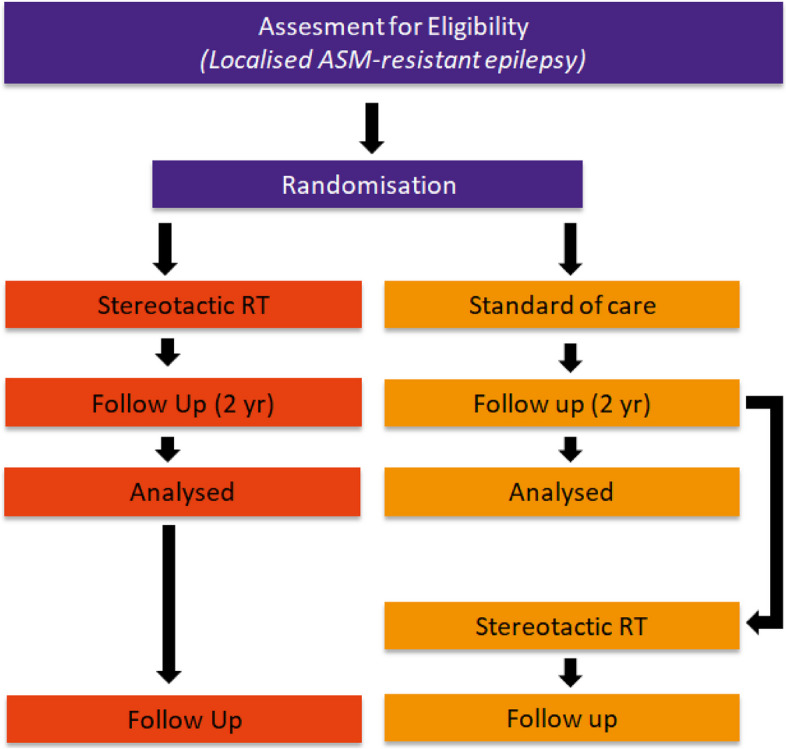
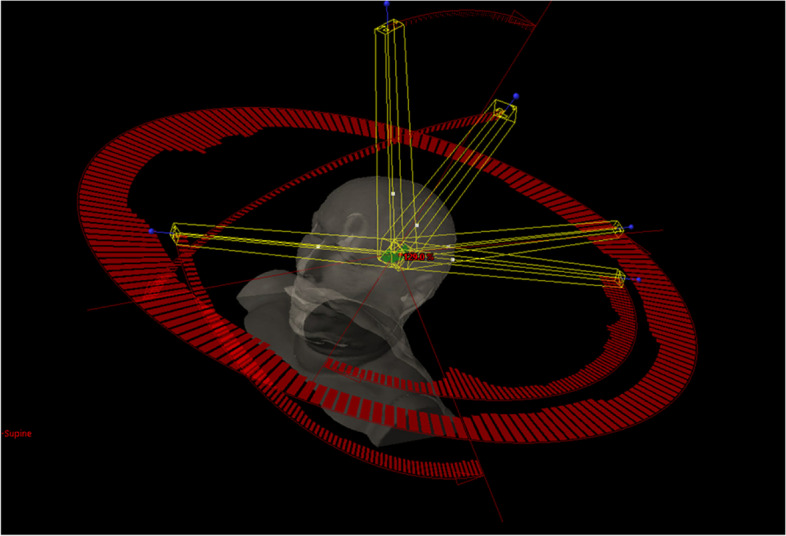
Methods: In this waitlist-controlled phase 3 clinical trial, participants are randomly assigned in a 1:1 ratio to either receive SRT as the intervention, while the standard treatments consist of ASM continuation and neuromodulation. After 2-year follow-up, patients randomized for the standard treatment (waitlist-control group) are offered SRT. Patients aged ≥ 18 years with focal DRE and a pretreatment defined epileptogenic zone (EZ) not eligible for open surgery will be included. The intervention is a LINAC-based single fraction (24 Gy) SRT treatment. The target volume is defined as the epileptogenic zone (EZ) on all (non) invasive examinations. The seizure frequency will be monitored on a daily basis using an electronic diary and an automatic seizure detection system during the night. Potential side effects are evaluated using advanced MRI, cognitive evaluation, Common Toxicity Criteria, and patient-reported outcome questionnaires. In addition, the cost-effectiveness of the SRT treatment will be evaluated.
Discussion: This is the first randomized trial comparing SRT with standard of care in patients with DRE, non-eligible for open surgery. The primary objective is to determine whether SRT significantly reduces the seizure frequency 2 years after treatment. The results of this trial can influence the current clinical practice and medical cost reimbursement in the Netherlands for patients with focal DRE who are not eligible for open surgery, providing a non-invasive curative treatment option.
Trial registration: Clinicaltrials.gov Identifier: NCT05182437. Registered on September 27, 2021.
Keywords: Cognition; Epilepsy; MRI; Radiosurgery; Stereotactic radiation therapy (SRT).
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- “Nivel Zorgregistraties eerste lijn.”. Available: https://www.volksgezondheidenzorg.info/onderwerp/epilepsie/cijfers-conte...
-
- Pixsil, “Epilepsiechirurgie,” Epilepsiefonds. Available: https://www.epilepsie.nl/over-epilepsie/pagina/101-2/epilepsiechirurgie. Accessed: 17 Mar 2021
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
