

Prevention of persistent pain with lidocaine infusions in breast cancer surgery (PLAN): study protocol for a multicenter randomized controlled trial
- PMID: 38773653
- PMCID: PMC11110187
- DOI: 10.1186/s13063-024-08151-4
Prevention of persistent pain with lidocaine infusions in breast cancer surgery (PLAN): study protocol for a multicenter randomized controlled trial
Abstract
Background: Persistent pain is a common yet debilitating complication after breast cancer surgery. Given the pervasive effects of this pain disorder on the patient and healthcare system, post-mastectomy pain syndrome (PMPS) is becoming a larger population health problem, especially as the prognosis and survivorship of breast cancer increases. Interventions that prevent persistent pain after breast surgery are needed to improve the quality of life of breast cancer survivors. An intraoperative intravenous lidocaine infusion has emerged as a potential intervention to decrease the incidence of PMPS. We aim to determine the definitive effects of this intervention in patients undergoing breast cancer surgery.
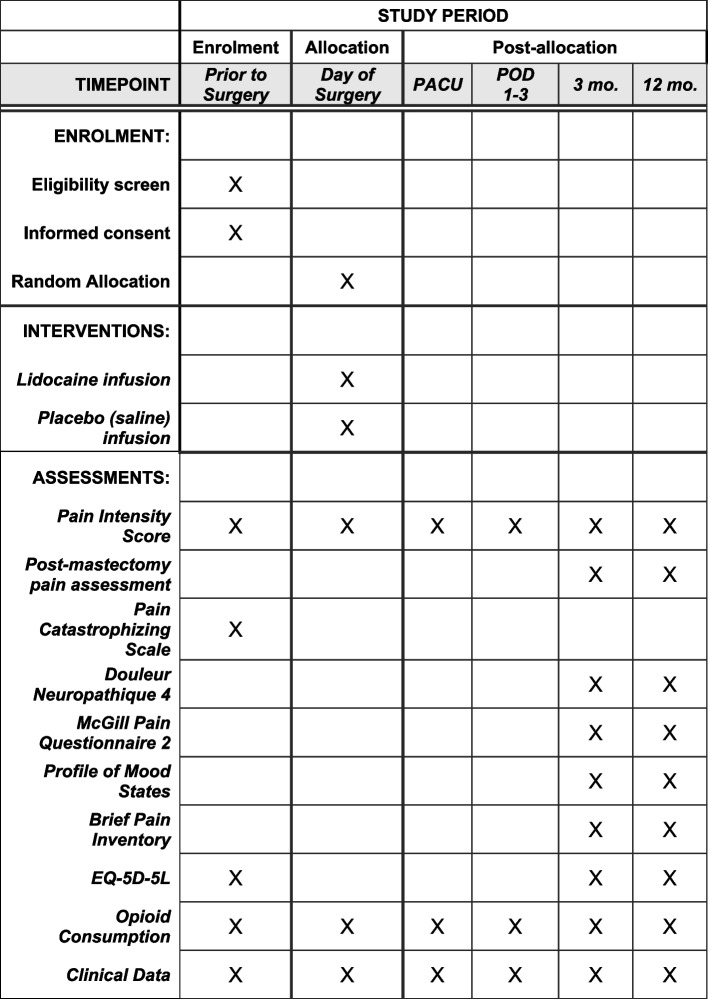
Methods: PLAN will be a multicenter, parallel-group, blinded, 1:1 randomized, placebo-controlled trial of 1,602 patients undergoing breast cancer surgery. Adult patients scheduled for a lumpectomy or mastectomy will be randomized to receive an intravenous 2% lidocaine bolus of 1.5 mg/kg with induction of anesthesia, followed by a 2.0 mg/kg/h infusion until the end of surgery, or placebo solution (normal saline) at the same volume. The primary outcome will be the incidence of persistent pain at 3 months. Secondary outcomes include the incidence of pain and opioid consumption at 1 h, 1-3 days, and 12 months after surgery, as well as emotional, physical, and functional parameters, and cost-effectiveness.
Discussion: This trial aims to provide definitive evidence on an intervention that could potentially prevent persistent pain after breast cancer surgery. If this trial is successful, lidocaine infusion would be integrated as standard of care in breast cancer management. This inexpensive, widely available, and easily administered intervention has the potential to reduce pain and suffering in an already afflicted patient population, decrease the substantial costs of chronic pain management, potentially decrease opioid use, and improve the quality of life in patients.
Trial registration: This trial has been registered on clinicaltrials.gov (NCT04874038, Dr. James Khan. Date of registration: May 5, 2021).
Keywords: Breast cancer surgery; Chronic pain; Chronic postsurgical pain; Lidocaine infusion; Perioperative care; Post-mastectomy pain syndrome.
© 2024. The Author(s).
Conflict of interest statement
JSK—Supported by a Merit award by the Department of Anesthesiology and Pain Medicine, Recipient of a fellowship awarded by Michael G. DeGroote Institute of Pain Research and Care which supported the initial pilot for this trial.
IG—reports consulting honoraria from Combigene, GW Research, Lilly and Novaremed.
KK—Supported in part by a merit award from the Department of Anesthesia and Pain Medicine, University of Toronto-Research support and/or consultancy for Octapharma and Instrumentation Laboratory.
KSL—Co-PI of an observational study on medical cannabis funded by Shoppers Drug Mart.
DWL—Consultant with Merck Canada Inc., Speaker fees from Mayo Clinic foundation (2022).
PR—Has received several Investigator Initiated Trial grants from companies who were funders of the trials whereas my research center was the sponsor. These grants had a contract between our attorneys of our research institution and companies to make sure the PI remained totally independent form companies who were only funders (no right on data, no right on publications). Gave educational lectures for companies and received some honorarium (Medtronic, Medasense Ltd, Merck, Avirpharma).
NJLK—Consultant for MOLLI Surgical.
JWB—Supported, in part, by a Canadian Institutes of Health Research Canada Research Chair in the prevention and management of chronic pain.
MS—Currently holds the Canadian Anesthesiologists’ Society Career Scientist Grant and a Merit award from the Department of Anesthesiology and Pain Medicine, University of Toronto (Toronto, Canada) to support academic time. Dr. Singh also serves on the Medical Advisory Board of Hypersomnia Foundation (Atlanta, GA) at a voluntary basis.
PJD—Has received grant funding from the following companies: Abbott Diagnostics, Roche Diagnostics, Siemens. He has received medical devices for trials from the following company: CloudDX. He is a consultant for: Abbott Canada, Renibus, Roche Canada, Trimedic. He is a member of advisory boards to: Bayer and Quidel. He was a speaker for the following company: Velocity.
Figures
References
-
- Reports H, Statistics Canada CC for HI. Canadian Cancer Statistics Advisory Committee in collaboration with the Canadian Cancer Society, Statistics Canada and the Public Health Agency of Canada. Canadian Cancer Statistics. Toronto: Canadian Cancer Society; 2021.
-
- Jung BF, Ahrendt GM, Oaklander AL, Dworkin RH. Neuropathic pain following breast cancer surgery: proposed classification and research update. PAID. 2003;104(1–2):1–13. - PubMed
-
- Schug SA, Lavand’homme P, Barke A, Korwisi B, Rief W, Treede RD, et al. The IASP classification of chronic pain for ICD-11: chronic postsurgical or posttraumatic pain. PAID. 2019;160(1):45–52. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
