

Treatment outcomes in patients with large B-cell lymphoma after progression to chimeric antigen receptor T-cell therapy
- PMID: 38774657
- PMCID: PMC11106798
- DOI: 10.1002/hem3.62
Treatment outcomes in patients with large B-cell lymphoma after progression to chimeric antigen receptor T-cell therapy
Abstract
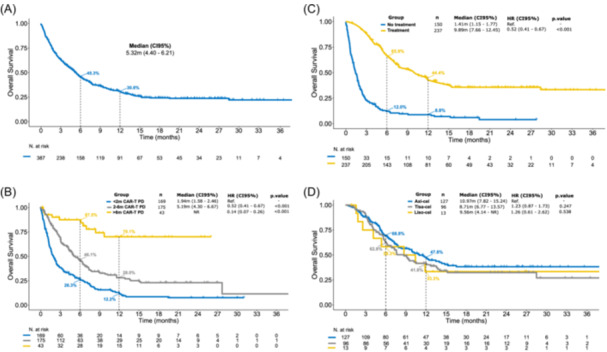
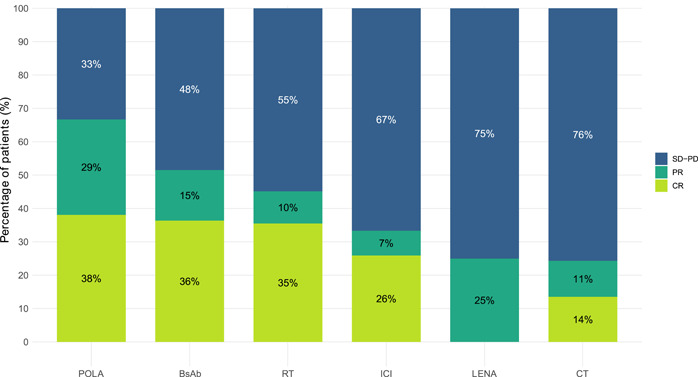
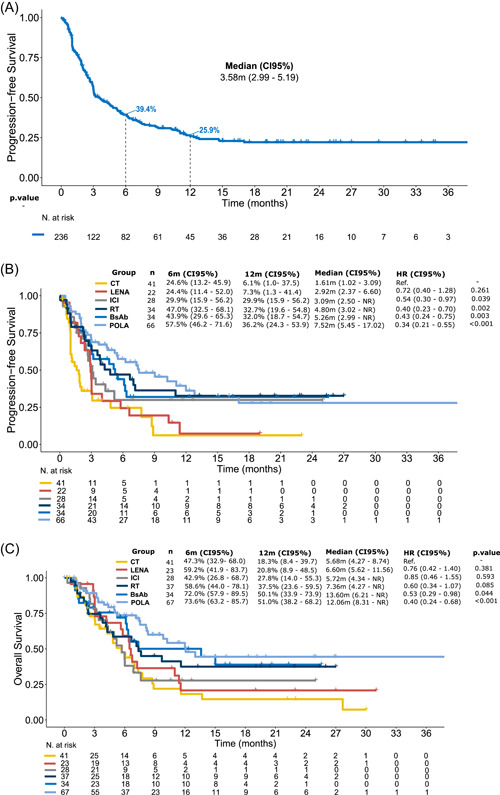
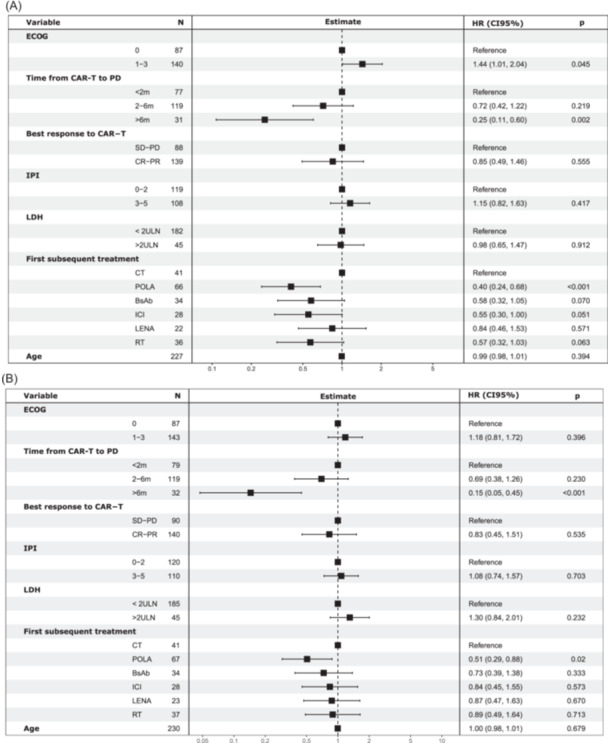
Over 60% of relapsed/refractory (R/R) large B-cell lymphoma (LBCL) patients who receive chimeric antigen receptor (CAR) T cells will experience disease progression. There is no standard next line of therapy and information in this setting is scarce and heterogeneous. We analyzed 387 R/R LBCL patients who progressed after CAR T cells from July 2018 until March 2022 in Spain and the United Kingdom. Median overall survival (OS) was 5.3 months, with significant differences according to the interval between infusion and progression (<2 months [1.9 months], 2-6 months [5.2 months], and >6 months [not reached]). After progression, 237 (61%) patients received treatment. Focusing on the first subsequent therapy, overall (complete) response rates were 67% (38%) for polatuzumab-bendamustine-rituximab (POLA), 51% (36%) for bispecific antibodies (BsAb), 45% (35%) for radiotherapy (RT), 33% (26%) for immune checkpoint inhibitors (ICIs), 25% (0%) for lenalidomide (LENA), and 25% (14%) for chemotherapy (CT). In terms of survival, 12-month progression-free survival and OS was 36.2% and 51.0% for POLA, 32.0% and 50.1% for BsAb, 30.8% and 37.5% for RT, 29.9% and 27.8% for ICI, 7.3% and 20.8% for LENA, and 6.1% and 18.3% for CT. Thirty-two (14%) patients received an allogeneic hematopoietic cell transplant with median OS not reached after a median follow-up of 15.1 months. In conclusion, patients with R/R LBCL who progress within the first 2 months after CAR T-cell therapy have dismal outcomes. Novel targeted agents, such as polatuzumab and BsAbs, can achieve prolonged survival after CAR T-cell therapy failure.
© 2024 The Authors. HemaSphere published by John Wiley & Sons Ltd. on behalf of European Hematology Association.
Conflict of interest statement
Gloria Iacoboni: Honoraria and travel support: Novartis, Kite/Gilead, Bristol‐Myers Squibb, Abbvie, Autolus, Sandoz, Miltenyi, and AstraZeneca. Maeve O'Reilly has served on advisory boards and received honoraria from Kite/Gilead and Novartis. Mi Kwon: Consulting and lectures: Gilead and Jazz, Pfizer. Javier Delgado: Honoraria from Kite‐Gilead, Novartis, Bristol Myers Squibb, and Janssen. Claire Roddie has served on advisory boards and received honoraria from Kite/Gilead, Novartis, and BMS. Manuel Guerreiro: Consultancy: Novartis, Kite, BMS, Pierre Fabre, and MSD. Alberto Mussetti: BMS: consultancy; Takeda: Honoraria; Gilead: Research Funding; Jazz Pharmaceuticals: Consultancy. Robin Sanderson: Kite/Gilead and Novartis—speakers fees, honoraria, conference travel. Sunil Iyengar: Abbvie—Conference support; Beigene—advisory board; BMS—Conference support; Janssen—Speaker fees; Kite—advisory board; Takeda—advisory board, speaker fees, and conference support. Juan‐Manuel Sancho: Honoraria as speaker in medical education activities from Roche, Gilead‐Kite, Celgene‐BMS, Janssen, Novartis, and Incyte. Honoraria as participant in advisory boards or consulting for Roche, Gilead‐Kite, Celgene‐BMS, Janssen, Novartis, Incyte, Lilly, Beigene, and Myltenyi Biomedicine. Pere Barba: Advisory board and consultancy: Allogene, Amgen, BMS/Celgene, Kite/Gilead, Incyte, Miltenyi Biomedicine, Novartis, Nektar, Pfizer, and Pierre Fabre. Rafael Hernani: Research: Gilead. Travel support: Gilead. Honoraria: Gilead, Janssen, MSD, Celgene, and Novartis. Anna Sureda: Honoraria from Takeda, BMS, Merck, Janssen, Sanofi, Roche, Novartis, and Gilead. Alejandro Martin Garcia‐Sancho: Consultancy for Roche, BMS/Celgene, Kyowa Kirin, Novartis, Gilead/Kite, Incyte, Lilly, ADC Therapeutics America, Miltenyi, Ideogen, Abbvie, and Sobi. Honorario from Roche, BMS/Celgene, Janssen, Gilead/Kite, Takeda, Eusa Pharma, and Abbvie. Pau Abrisqueta: consulting/advisory: Roche, Genmab, Janssen, BMS, AbbVie, AstraZeneca, BeiGene; Honoraria: Roche, Genmab, Janssen, BMS, AbbVie, AstraZeneca, Gilead, and Incyte. Andrea Kuhnl has served on advisory boards and received honoraria from Kite/Gilead, Novartis, and BMS. The remaining authors declare no conflict of interest.
Figures
References
-
- Schuster SJ, Tam CS, Borchmann P, et al. Long‐term clinical outcomes of tisagenlecleucel in patients with relapsed or refractory aggressive B‐cell lymphomas (JULIET): a multicentre, open‐label, single‐arm, phase 2 study. Lancet Oncol. 2021;22(10):1403‐1415. - PubMed