

Deep Learning for Breast Cancer Risk Prediction: Application to a Large Representative UK Screening Cohort
- PMID: 38775671
- PMCID: PMC11294956
- DOI: 10.1148/ryai.230431
Deep Learning for Breast Cancer Risk Prediction: Application to a Large Representative UK Screening Cohort
Abstract
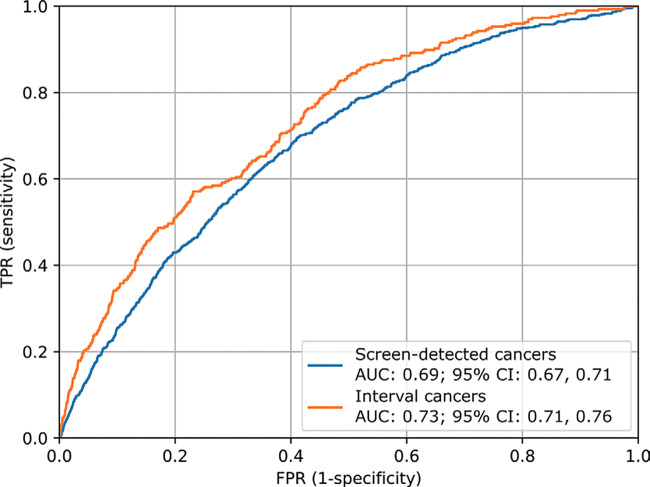
Purpose To develop an artificial intelligence (AI) deep learning tool capable of predicting future breast cancer risk from a current negative screening mammographic examination and to evaluate the model on data from the UK National Health Service Breast Screening Program. Materials and Methods The OPTIMAM Mammography Imaging Database contains screening data, including mammograms and information on interval cancers, for more than 300 000 female patients who attended screening at three different sites in the United Kingdom from 2012 onward. Cancer-free screening examinations from women aged 50-70 years were performed and classified as risk-positive or risk-negative based on the occurrence of cancer within 3 years of the original examination. Examinations with confirmed cancer and images containing implants were excluded. From the resulting 5264 risk-positive and 191 488 risk-negative examinations, training (n = 89 285), validation (n = 2106), and test (n = 39 351) datasets were produced for model development and evaluation. The AI model was trained to predict future cancer occurrence based on screening mammograms and patient age. Performance was evaluated on the test dataset using the area under the receiver operating characteristic curve (AUC) and compared across subpopulations to assess potential biases. Interpretability of the model was explored, including with saliency maps. Results On the hold-out test set, the AI model achieved an overall AUC of 0.70 (95% CI: 0.69, 0.72). There was no evidence of a difference in performance across the three sites, between patient ethnicities, or across age groups. Visualization of saliency maps and sample images provided insights into the mammographic features associated with AI-predicted cancer risk. Conclusion The developed AI tool showed good performance on a multisite, United Kingdom-specific dataset. Keywords: Deep Learning, Artificial Intelligence, Breast Cancer, Screening, Risk Prediction Supplemental material is available for this article. ©RSNA, 2024.
Keywords: Artificial Intelligence; Breast Cancer; Deep Learning; Risk Prediction; Screening.
Conflict of interest statement
Figures






References
-
- Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer . National Institute for Health and Care Excellence . 2013. . https://www.nice.org.uk/guidance/cg164/ifp/chapter/How-breast-cancer-ris.... Published June 25, 2013. Last updated November 14, 2023. Accessed March 19, 2023 . - PubMed
-
- Monticciolo DL , Newell MS , Hendrick RE , et al . Breast cancer screening for average-risk women: recommendations from the ACR Commission on Breast Imaging . J Am Coll Radiol 2017. ; 14 ( 9 ): 1137 – 1143 . - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
