

Pharmacodynamic changes in tumor and immune cells drive iberdomide's clinical mechanisms of activity in relapsed and refractory multiple myeloma
- PMID: 38776914
- PMCID: PMC11228401
- DOI: 10.1016/j.xcrm.2024.101571
Pharmacodynamic changes in tumor and immune cells drive iberdomide's clinical mechanisms of activity in relapsed and refractory multiple myeloma
Abstract
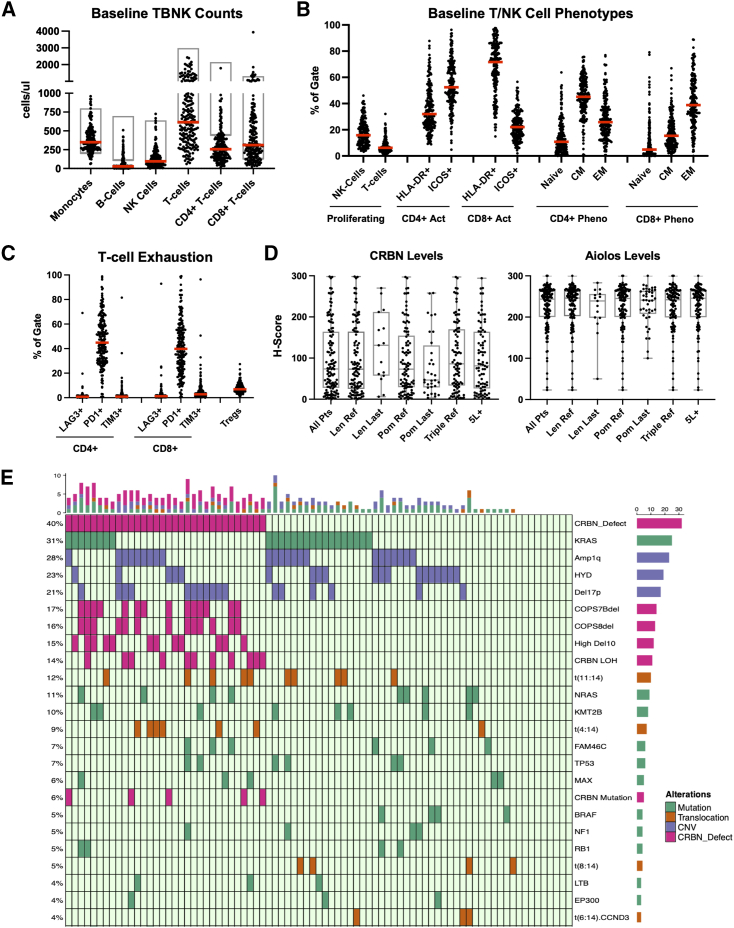
Iberdomide is a next-generation cereblon (CRBN)-modulating agent in the clinical development in multiple myeloma (MM). The analysis of biomarker samples from relapsed/refractory patients enrolled in CC-220-MM-001 (ClinicalTrials.gov: NCT02773030), a phase 1/2 study, shows that iberdomide treatment induces significant target substrate degradation in tumors, including in immunomodulatory agent (IMiD)-refractory patients or those with low CRBN levels. Additionally, some patients with CRBN genetic dysregulation who responded to iberdomide have a similar median progression-free survival (PFS) (10.9 months) and duration of response (DOR) (9.5 months) to those without CRBN dysregulation (11.2 month PFS, 9.4 month DOR). Iberdomide treatment promotes a cyclical pattern of immune stimulation without causing exhaustion, inducing a functional shift in T cells toward an activated/effector memory phenotype, including in triple-class refractory patients and those receiving IMiDs as a last line of therapy. This analysis demonstrates that iberdomide's clinical mechanisms of action are driven by both its cell-autonomous effects overcoming CRBN dysregulation in MM cells, and potent immune stimulation that augments anti-tumor immunity.
Keywords: CC-220; IMiD refractory; cereblon; iberdomide; immune stimulatory; myeloma.
Copyright © 2024. Published by Elsevier Inc.
Conflict of interest statement
Declaration of interests M.A., E.F., M.W., M.O., N.S., P.M., T.P., P.R., and A.T. report equity ownership in Bristol Myers Squib. M.A., E.F., N.S., M.W., M.O., P.M., T.P., and P.R. are current employees of Bristol Myers Squib. A.T. is a former employee of Bristol Myers Squibb. Funding for data generation, processing, and storage was provided by Bristol Myers Squib. S.L. reports consulting fees from AbbVie, Bristol Myers Squibb, GlaxoSmithKline, Janssen Pharmaceuticals, and Takeda; institution grants or contracts from Bristol Myers Squibb, Janssen, and Takeda; membership on an entity’s board of directors or advisory committees for TG Therapeutics; and stock ownership in TG Therapeutics. N.W.C.J.v.d.D. reports institution grants or contracts from Amgen, Cellectis, and Janssen Pharmaceuticals and membership on an entity’s board of directors or advisory committees for Adaptive Biotechnologies, Amgen, GlaxoSmithKline, Janssen Pharmaceuticals, Novartis, Roche Sanofi, and Takeda. S.P. reports consulting fees from Foundation Medicine and research funding from Bristol Myers Squibb (Celgene), Karyopharm, and Amgen. P.R. reports shares in Doloromics.
Figures





References
-
- Lonial S., Popat R., Hulin C., Jagannath S., Oriol A., Richardson P.G., Facon T., Weisel K., Larsen J.T., Minnema M.C., et al. Iberdomide plus dexamethasone in heavily pretreated late-line relapsed or refractory multiple myeloma (CC-220-MM-001): a multicentre, multicohort, open-label, phase 1/2 trial. Lancet. Haematol. 2022;9:e822–e832. - PubMed
-
- Bjorklund C.C., Lu L., Kang J., Hagner P.R., Havens C.G., Amatangelo M., Wang M., Ren Y., Couto S., Breider M., et al. Rate of CRL4CRBN substrate Ikaros and Aiolos degradation underlies differential activity of lenalidomide and pomalidomide in multiple myeloma cells by regulation of c-Myc and IRF4. Blood Cancer J. 2015;5:e354. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
