

Screening of substance use in pregnancy: A Danish cross-sectional study
- PMID: 38778571
- PMCID: PMC11168282
- DOI: 10.1111/aogs.14862
Screening of substance use in pregnancy: A Danish cross-sectional study
Abstract
Introduction: There is a paucity of objectively verified data on substance use among Danish pregnant women. We estimated the prevalence of substance use including alcohol and nicotine among the general population of Danish pregnant women.
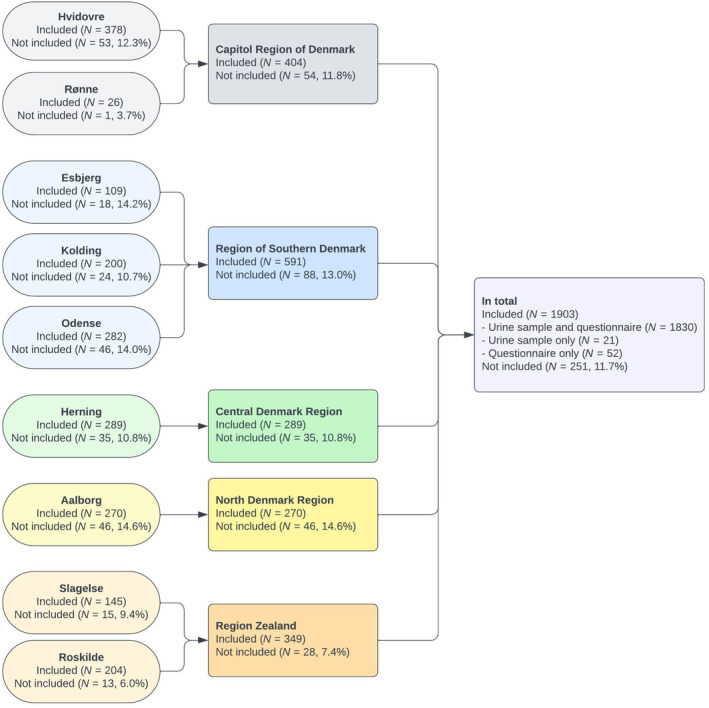
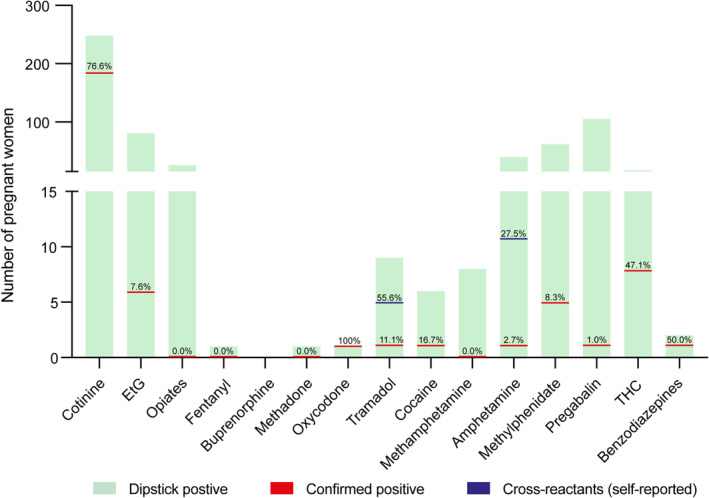
Material and methods: In this anonymous, national, cross-sectional, descriptive study, pregnant women were invited when attending an ultrasound scan between November 2019 and December 2020 at nine Danish hospitals. Women submitted a urine sample and filled out a questionnaire. Urine samples were screened on-site with a qualitative urine dipstick for 15 substances including alcohol, nicotine, opioids, amphetamines, cannabis, and benzodiazepines. All screen-positive urine samples underwent secondary quantitative analyses with gold standard, liquid chromatography-tandem mass spectrometry (LC-MS/MS) analysis. Results were compared to questionnaire information to analyze the validity of self-reporting and to examine possible cross-reactions.
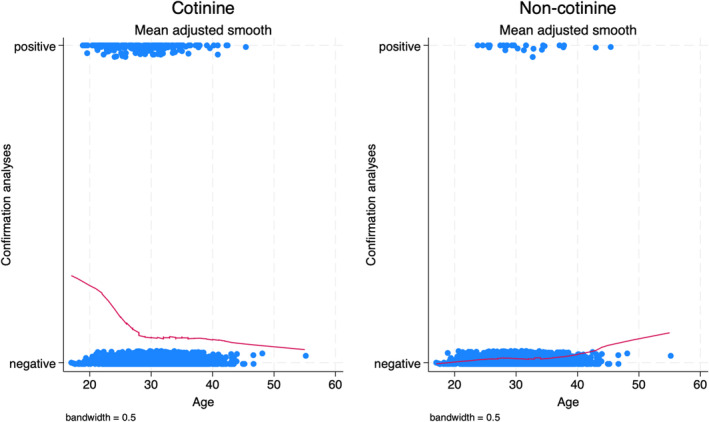
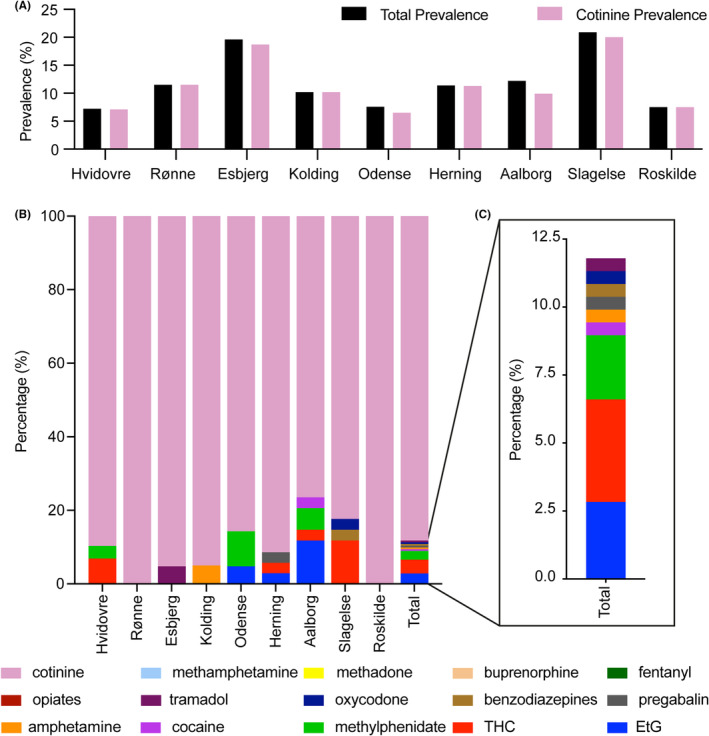
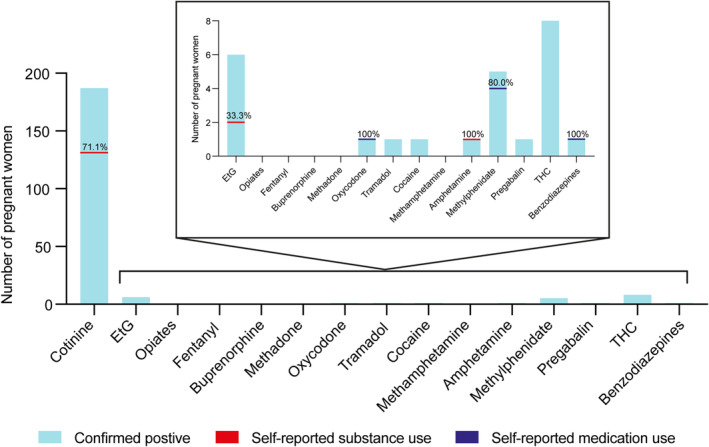
Results: A total of 1903 of 2154 invited pregnant women participated (88.3%). The prevalence of dipstick-positive urine samples was 25.0%. 44.0% of these were confirmed positive, resulting in a total confirmed prevalence of 10.8%. The prevalence of nicotine use was 10.1%-and for all other substances, <0.5%. Nicotine use was more prevalent among younger pregnant women, while other substance use appeared evenly distributed over age groups. Self-reporting of use of nicotine products was high (71.1%), but low for cannabis and alcohol intake (0% and 33.3%, respectively). Prescription medication explained almost all cases of oxycodone, methylphenidate, and benzodiazepine use.
Conclusions: Substance use among pregnant women consisted mainly of nicotine. Dipstick screening involved risks of false negatives and false positives. Except for alcohol intake and cannabis use, dipstick analyses did not seem to provide further information than self-reporting. LC-MS/MS analyses remain gold standard, and future role of dipstick screenings should be discussed.
Keywords: alcohol; cannabis; high risk pregnancy; maternal–fetal medicine; maternity care; neonatology; pregnancy; prenatal care; substance use.
© 2024 The Authors. Acta Obstetricia et Gynecologica Scandinavica published by John Wiley & Sons Ltd on behalf of Nordic Federation of Societies of Obstetrics and Gynecology (NFOG).
Conflict of interest statement
None.
Figures

References
-
- Makarious L, Teng A, Oei JL. SIDS is associated with prenatal drug use: a meta‐analysis and systematic review of 4 238 685 infants. Arch Dis Child Fetal Neonatal Ed. 2022;107:617‐623. - PubMed
-
- Pereira PP, Da Mata FA, Figueiredo AC, de Andrade KR, Pereira MG. Maternal active smoking during pregnancy and low birth weight in the Americas: a systematic review and meta‐analysis. Nicotine Tob Res. 2017;19(5):497‐505. - PubMed
-
- Broccia M, Hansen BM, Winckler JM, et al. Heavy prenatal alcohol exposure and obstetric and birth outcomes: a Danish nationwide cohort study from 1996 to 2018. Lancet Public Health. 2023;8:e28‐e35. - PubMed
-
- Singh S, Filion KB, Abenhaim HA, Eisenberg MJ. Prevalence and outcomes of prenatal recreational cannabis use in high‐income countries: a scoping review. BJOG. 2020;127:8‐16. - PubMed
