

Usability of serum AIM2 as a predictive biomarker of stroke-associated pneumonia and poor prognosis after acute supratentorial intracerebral hemorrhage: A prospective longitudinal cohort study
- PMID: 38778966
- PMCID: PMC11109811
- DOI: 10.1016/j.heliyon.2024.e31007
Usability of serum AIM2 as a predictive biomarker of stroke-associated pneumonia and poor prognosis after acute supratentorial intracerebral hemorrhage: A prospective longitudinal cohort study
Abstract
Background: Absent in melanoma 2 (AIM2) is implicated in inflammatory processes. We measured serum AIM2 with intent to unveil its predictive significance for stroke-associated pneumonia (SAP) and functional prognosis following acute intracerebral hemorrhage (ICH).
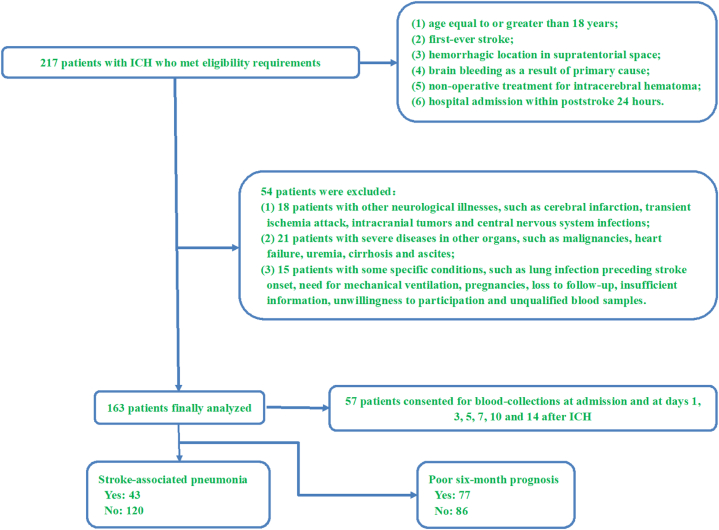
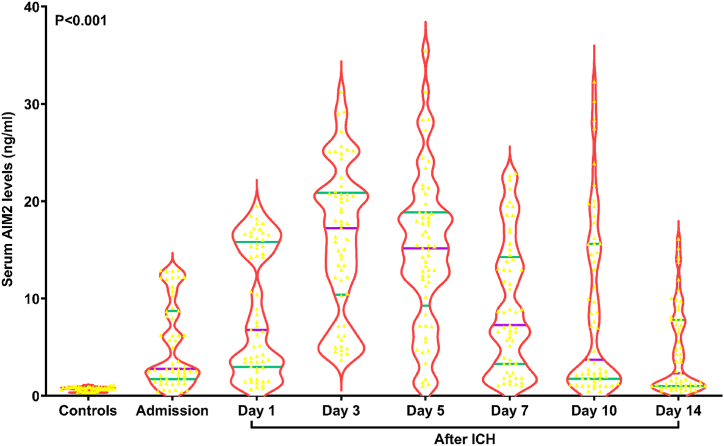
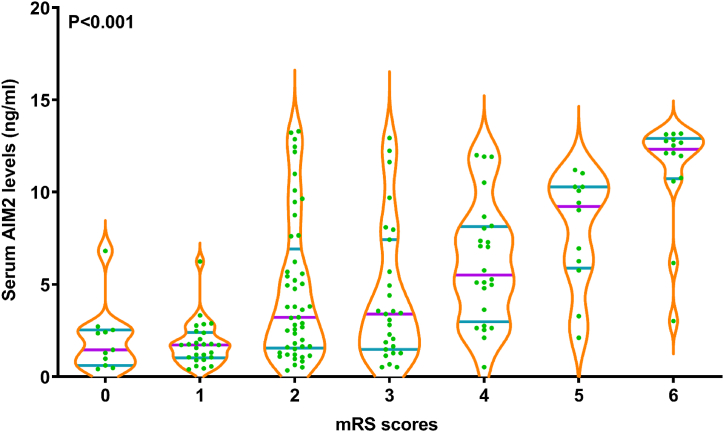
Methods: In this prospective cohort study, serum AIM2 concentrations of 163 ICH patients were gauged upon admission and 57 of them also consented for measurements at days 1, 3, 5, 7, 10 and 14. Coupled with 57 individuals without health conditions, dynamic change of serum AIM2 levels were uncovered. National Institutes of Health Stroke Scale (NIHSS) scores and hematoma volume were identified as the dual indicators of severity. Poststroke six-month modified Rankin Scale (mRS) scores ranging from 3 to 6 indicated an unfavorable outcome. SAP was observed during the first seven days after ICH. Sequential univariate and multivariate analyses were performed to discern predictors of SAP and adverse prognosis.
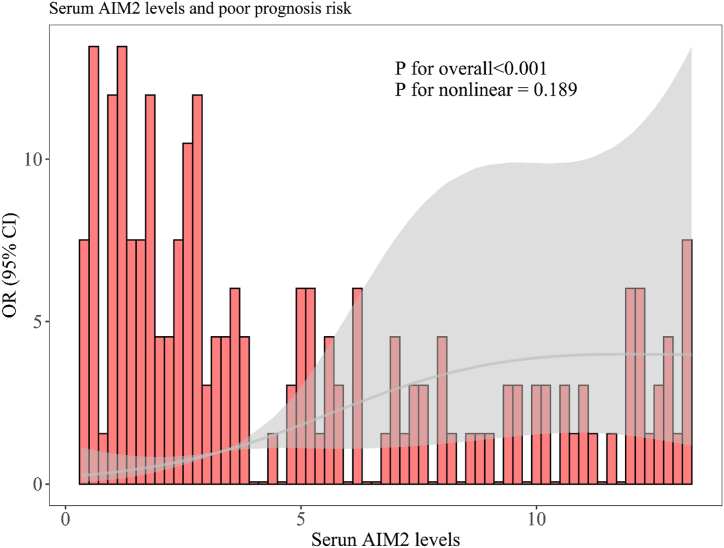
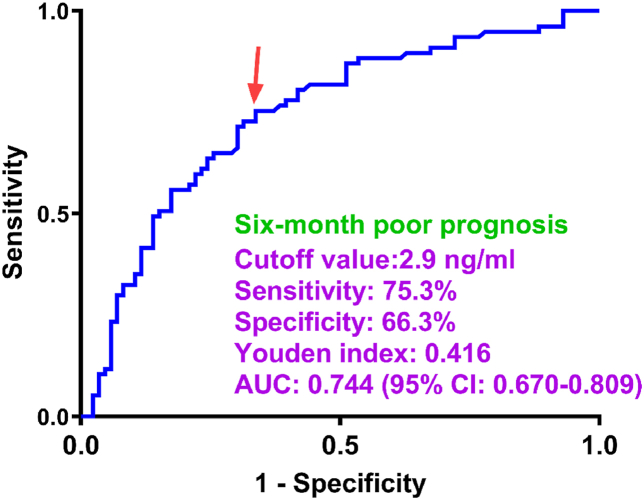
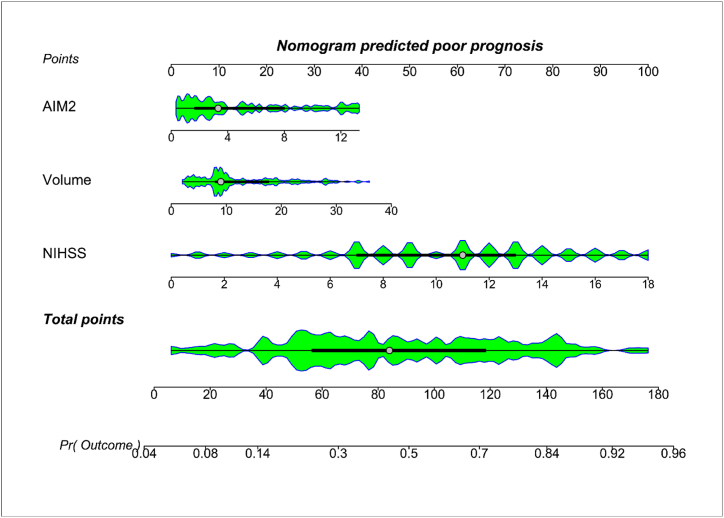
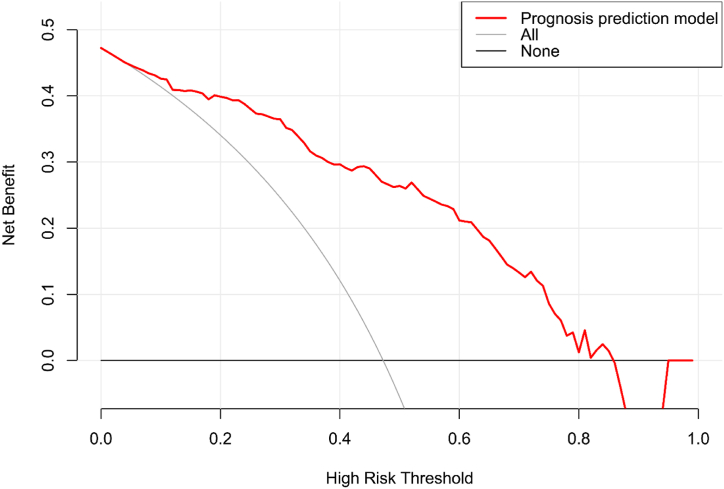
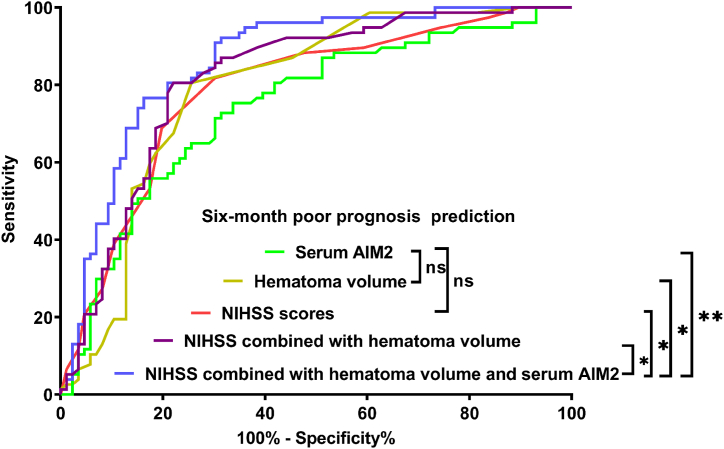
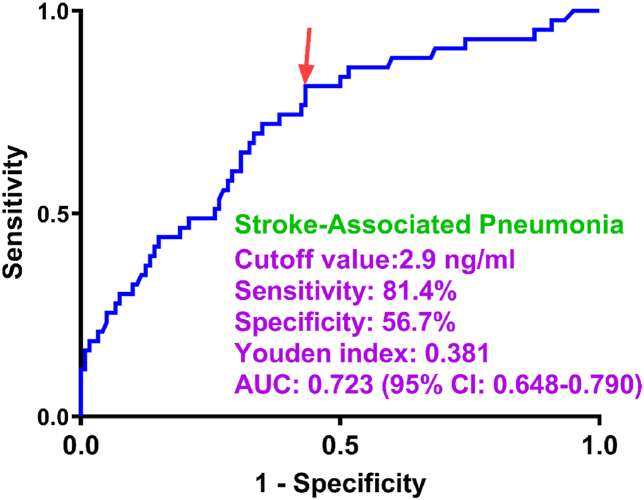
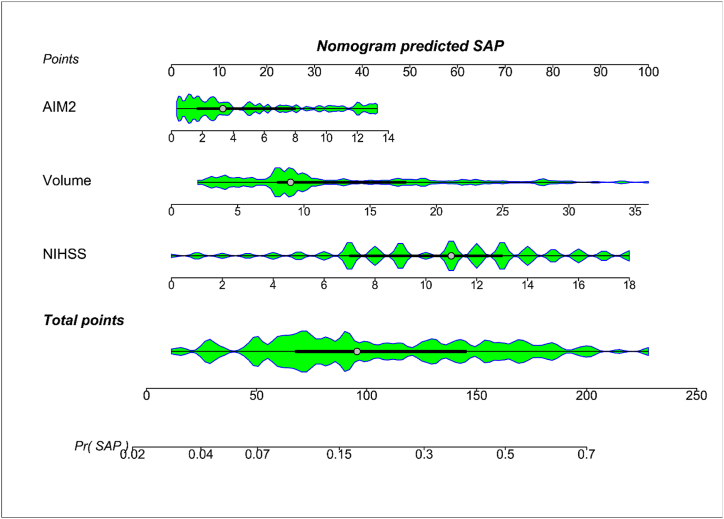
Results: The serum levels of AIM2 in patients exhibited a marked elevation upon admission, reaching peak levels on the third and fifth days, and remained notably elevated until day 14 compared to those of the control group. Serum AIM2 levels showed independent correlations with both NIHSS scores and the volume of hematoma. Additionally, AIM2 concentrations were independently associated with a poor prognosis and SAP at the six-month mark. Within the framework of restricted cubic spline analysis, serum AIM2 concentrations exhibited a linear correlation with the likelihood of developing SAP and experiencing a poor prognosis. In the context of receiver operating characteristic (ROC) curve analysis, serum AIM2 concentrations effectively differentiated risks of SAP and poor prognosis. By employing segmented analysis, serum AIM2 concentrations showed negligible interactions with several traditional variables, such as age, gender, smoking habits, alcohol consumption, and more. The integrated model incorporating serum AIM2, NIHSS scores, and the volume of hematoma was depicted by employing a nomogram and demonstrated strong predictive performance for poor prognosis or SAP across various evaluation metrics, including ROC curve analysis, calibration curve analysis, and decision curve analysis.
Conclusion: Serum AIM2 levels show a marked increase shortly after intracerebral hemorrhage (ICH), which may accurately reflect stroke severity, and effectively predict SAP and poor neurological outcomes, and therefore serum AIM2 stands out as an encouraging predictive indicator for ICH.
Keywords: Absent in melanoma 2; Biomarkers; Intracerebral hemorrhage; Prognosis; Severity; Stroke-associated pneumonia.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paperThe authors declare the following financial interests/personal relationships which may be considered as potential competing interests: Ping Li reports financial support was provided by Clinical Research Fund Project of Zhejiang Medical Association (2021ZYC-A210). If there are other authors, they declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures






Similar articles
-
RVD2 emerges as a serological marker in relation to severity and six-month clinical outcome following acute intracerebral hemorrhage: A prospective cohort study from a single academic institution.Clin Chim Acta. 2025 Jan 15;565:119988. doi: 10.1016/j.cca.2024.119988. Epub 2024 Oct 3. Clin Chim Acta. 2025. PMID: 39368689
-
A prospective cohort study on serum PINK1 as a biochemical marker in relation to poor neurological prognosis, stroke-associated pneumonia and early neurological deterioration after acute intracerebral hemorrhage.Clin Chim Acta. 2025 Jun 1;573:120282. doi: 10.1016/j.cca.2025.120282. Epub 2025 Apr 6. Clin Chim Acta. 2025. PMID: 40199435
-
Feasibility of Serum Peroxiredoxin 2 as a Biochemical Indicator for Reflecting Severity and Prognosticating Stroke-Associated Pneumonia, Early Neurological Deterioration and Poor Neurological Outcomes in Acute Supratentorial Intracerebral Hemorrhage: An Observational Analytical Clinical Study.Neuropsychiatr Dis Treat. 2025 Mar 20;21:621-640. doi: 10.2147/NDT.S505346. eCollection 2025. Neuropsychiatr Dis Treat. 2025. PMID: 40134763 Free PMC article.
-
Predictive Nomogram for Unfavorable Outcome of Spontaneous Intracerebral Hemorrhage.World Neurosurg. 2022 Aug;164:e1111-e1122. doi: 10.1016/j.wneu.2022.05.111. Epub 2022 May 30. World Neurosurg. 2022. PMID: 35654327 Review.
-
Advancements in prognostic markers and predictive models for intracerebral hemorrhage: from serum biomarkers to artificial intelligence models.Neurosurg Rev. 2024 Jul 31;47(1):382. doi: 10.1007/s10143-024-02635-2. Neurosurg Rev. 2024. PMID: 39083096 Review.
References
LinkOut - more resources
Full Text Sources
Miscellaneous
