

Clinician Perceptions on Using Decision Tools to Support Prediction-Based Shared Decision Making for Lung Cancer Screening
- PMID: 38779527
- PMCID: PMC11110512
- DOI: 10.1177/23814683241252786
Clinician Perceptions on Using Decision Tools to Support Prediction-Based Shared Decision Making for Lung Cancer Screening
Abstract
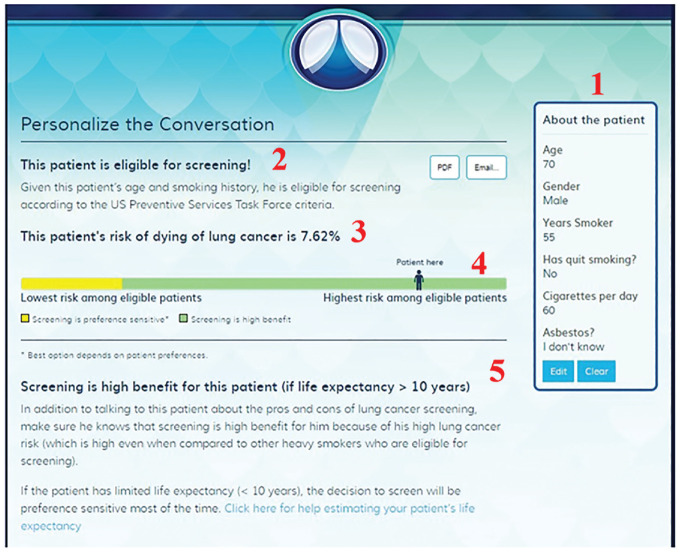
Background: Considering a patient's full risk factor profile can promote personalized shared decision making (SDM). One way to accomplish this is through encounter tools that incorporate prediction models, but little is known about clinicians' perceptions of the feasibility of using these tools in practice. We examined how clinicians react to using one such encounter tool for personalizing SDM about lung cancer screening (LCS).
Design: We conducted a qualitative study based on field notes from academic detailing visits during a multisite quality improvement program. The detailer engaged one-on-one with 96 primary care clinicians across multiple Veterans Affairs sites (7 medical centers and 6 outlying clinics) to get feedback on 1) the rationale for prediction-based LCS and 2) how to use the DecisionPrecision (DP) encounter tool with eligible patients to personalize LCS discussions.
Results: Thematic content analysis from detailing visit data identified 6 categories of clinician willingness to use the DP tool to personalize SDM for LCS (adoption potential), varying from "Enthusiastic Potential Adopter" (n = 18) to "Definite Non-Adopter" (n = 16). Many clinicians (n = 52) articulated how they found the concept of prediction-based SDM highly appealing. However, to varying degrees, nearly all clinicians identified challenges to incorporating such an approach in routine practice.
Limitations: The results are based on the clinician's initial reactions rather than longitudinal experience.
Conclusions: While many primary care clinicians saw real value in using prediction to personalize LCS decisions, more support is needed to overcome barriers to using encounter tools in practice. Based on these findings, we propose several strategies that may facilitate the adoption of prediction-based SDM in contexts such as LCS.
Highlights: Encounter tools that incorporate prediction models promote personalized shared decision making (SDM), but little is known about clinicians' perceptions of the feasibility of using these tools in practice.We examined how clinicians react to using one such encounter tool for personalizing SDM about lung cancer screening (LCS).While many clinicians found the concept of prediction-based SDM highly appealing, nearly all clinicians identified challenges to incorporating such an approach in routine practice.We propose several strategies to overcome adoption barriers and facilitate the use of prediction-based SDM in contexts such as LCS.
Keywords: academic detailing; lung cancer screening; shared decision making.
© The Author(s) 2024.
Conflict of interest statement
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors report grants from VA QUERI during the conduct of the study. Drs. Caverly and Lowery and Ms. Skurla reports grants from VA HSR&D during the conduct of the study. Dr. Wiener serves as deputy chief consultant for the VA National Center for Lung Cancer Screening. In addition, Dr. Caverly has a patent Apache 2.0 issued.
Figures
Similar articles
-
Implementation of a Web-Based Tool for Shared Decision-making in Lung Cancer Screening: Mixed Methods Quality Improvement Evaluation.JMIR Hum Factors. 2022 Apr 1;9(2):e32399. doi: 10.2196/32399. JMIR Hum Factors. 2022. PMID: 35363144 Free PMC article.
-
What Exactly Is Shared Decision-Making? A Qualitative Study of Shared Decision-Making in Lung Cancer Screening.J Gen Intern Med. 2020 Feb;35(2):546-553. doi: 10.1007/s11606-019-05516-3. Epub 2019 Nov 19. J Gen Intern Med. 2020. PMID: 31745852 Free PMC article.
-
Veterans' Lung Cancer Risk Conceptualizations versus Lung Cancer Screening Shared Decision-Making Conversations with Clinicians: A Qualitative Study.Med Decis Making. 2025 Jan;45(1):86-96. doi: 10.1177/0272989X241292643. Epub 2024 Nov 22. Med Decis Making. 2025. PMID: 39575828
-
The American Cancer Society National Lung Cancer Roundtable strategic plan: Current challenges and future directions for shared decision making for lung cancer screening.Cancer. 2024 Dec 1;130(23):3996-4011. doi: 10.1002/cncr.35382. Epub 2024 Sep 20. Cancer. 2024. PMID: 39302231 Review.
-
Shared decision-making conversations and smoking cessation interventions: critical components of low-dose CT lung cancer screening programs.Transl Lung Cancer Res. 2018 Jun;7(3):254-271. doi: 10.21037/tlcr.2018.05.10. Transl Lung Cancer Res. 2018. PMID: 30050764 Free PMC article. Review.
Cited by
-
The implementation challenge of computerised clinical decision support systems for the detection of disease in primary care: systematic review and recommendations.Implement Sci. 2025 Jul 17;20(1):33. doi: 10.1186/s13012-025-01445-4. Implement Sci. 2025. PMID: 40671071 Free PMC article.
References
LinkOut - more resources
Full Text Sources
