

Influence of Polygenic Background on the Clinical Presentation of Familial Hypercholesterolemia
- PMID: 38779854
- PMCID: PMC11208056
- DOI: 10.1161/ATVBAHA.123.320287
Influence of Polygenic Background on the Clinical Presentation of Familial Hypercholesterolemia
Abstract
Background: Heterozygous familial hypercholesterolemia (FH) is among the most common genetic conditions worldwide that affects ≈ 1 in 300 individuals. FH is characterized by increased levels of low-density lipoprotein cholesterol (LDL-C) and increased risk of coronary artery disease (CAD), but there is a wide spectrum of severity within the FH population. This variability in expression is incompletely explained by known risk factors. We hypothesized that genome-wide genetic influences, as represented by polygenic risk scores (PRSs) for cardiometabolic traits, would influence the phenotypic severity of FH.
Methods: We studied individuals with clinically diagnosed FH (n=1123) from the FH Canada National Registry, as well as individuals with genetically identified FH from the UK Biobank (n=723). For all individuals, we used genome-wide gene array data to calculate PRSs for CAD, LDL-C, lipoprotein(a), and other cardiometabolic traits. We compared the distribution of PRSs in individuals with clinically diagnosed FH, genetically diagnosed FH, and non-FH controls and examined the association of the PRSs with the risk of atherosclerotic cardiovascular disease.
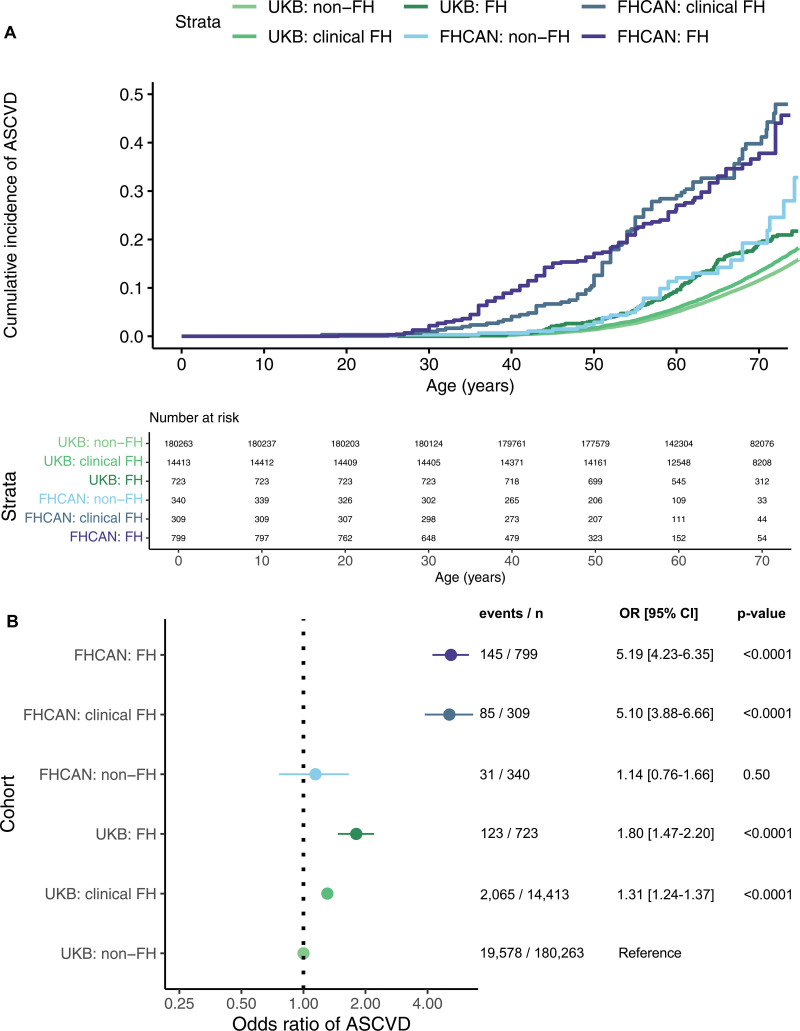
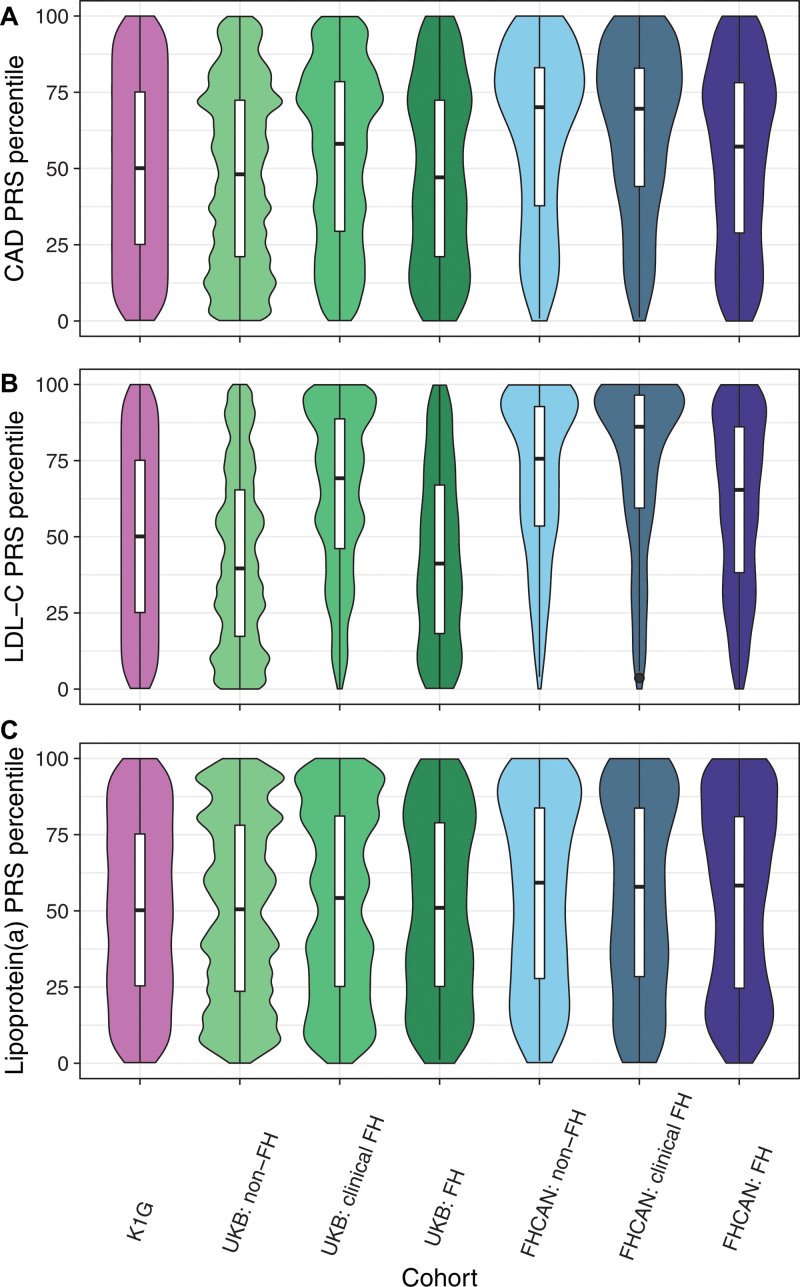
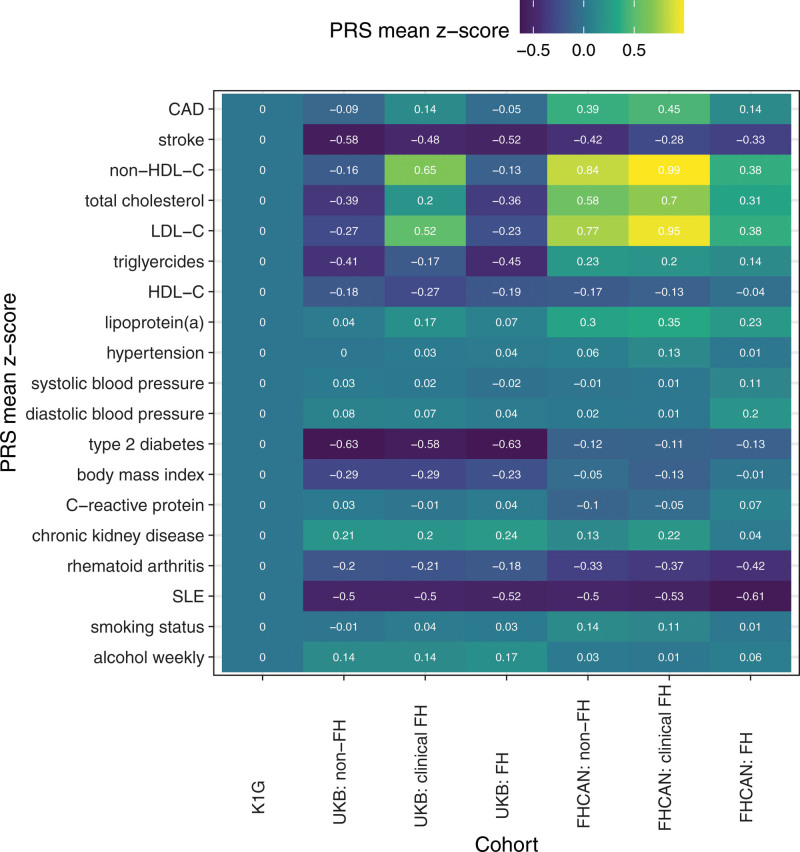
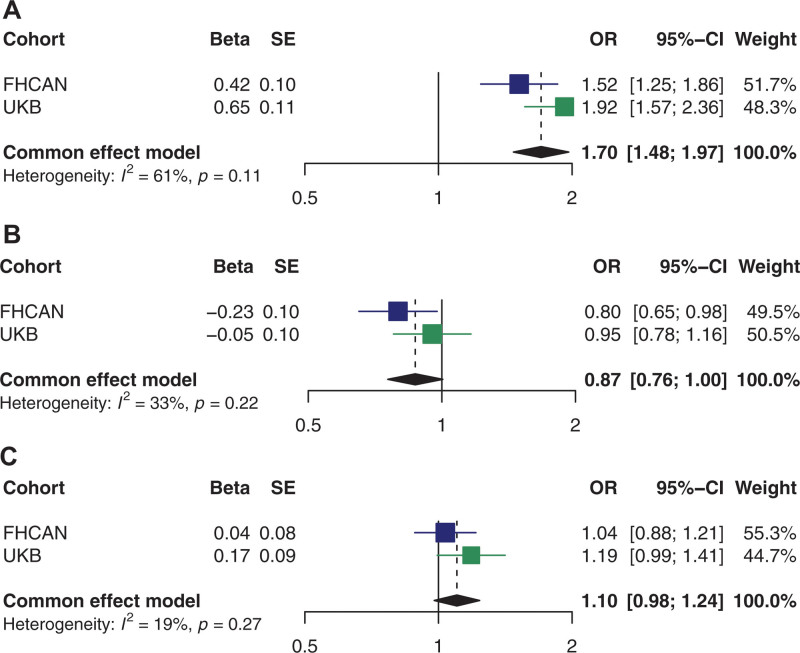
Results: Individuals with clinically diagnosed FH had higher levels of LDL-C, and the incidence of atherosclerotic cardiovascular disease was higher in individuals with clinically diagnosed compared with genetically identified FH. Individuals with clinically diagnosed FH displayed enrichment for higher PRSs for CAD, LDL-C, and lipoprotein(a) but not for other cardiometabolic risk factors. The CAD PRS was associated with a risk of atherosclerotic cardiovascular disease among individuals with an FH-causing genetic variant.
Conclusions: Genetic background, as expressed by genome-wide PRSs for CAD, LDL-C, and lipoprotein(a), influences the phenotypic severity of FH, expanding our understanding of the determinants that contribute to the variable expressivity of FH. A PRS for CAD may aid in risk prediction among individuals with FH.
Keywords: biological specimen banks; cardiovascular diseases; cholesterol, LDL; coronary artery disease; genetic risk score.
Conflict of interest statement
Figures
References
-
- Beheshti SO, Madsen CM, Varbo A, Nordestgaard BG. Worldwide prevalence of familial hypercholesterolemia: meta-analyses of 11 million subjects. J Am Coll Cardiol. 2020;75:2553–2566. doi: 10.1016/j.jacc.2020.03.057 - PubMed
-
- Hu P, Dharmayat KI, Stevens CAT, Sharabiani MTA, Jones RS, Watts GF, Genest J, Ray KK, Vallejo-Vaz AJ. Prevalence of familial hypercholesterolemia among the general population and patients with atherosclerotic cardiovascular disease: a systematic review and meta-analysis. Circulation. 2020;141:1742–1759. doi: 10.1161/CIRCULATIONAHA.119.044795 - PubMed
-
- Wang J, Dron JS, Ban MR, Robinson JF, McIntyre AD, Alazzam M, Zhao PJ, Dilliott AA, Cao H, Huff MW, et al. . Polygenic versus monogenic causes of hypercholesterolemia ascertained clinically. Arterioscler Thromb Vasc Biol. 2016;36:2439–2445. doi: 10.1161/ATVBAHA.116.308027 - PubMed
-
- Talmud PJ, Shah S, Whittall R, Futema M, Howard P, Cooper JA, Harrison SC, Li K, Drenos F, Karpe F, et al. . Use of low-density lipoprotein cholesterol gene score to distinguish patients with polygenic and monogenic familial hypercholesterolaemia: a case-control study. Lancet. 2013;381:1293–1301. doi: 10.1016/S0140-6736(12)62127-8 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
