

Kidney Transplant Outcomes From Deceased Donors Who Received Dialysis
- PMID: 38780515
- PMCID: PMC11117155
- DOI: 10.1001/jama.2024.8469
Kidney Transplant Outcomes From Deceased Donors Who Received Dialysis
Abstract
Importance: Recipient outcomes after kidney transplant from deceased donors who received dialysis prior to kidney donation are not well described.
Objective: To compare outcomes of transplant recipients who received kidneys from deceased donors who underwent dialysis prior to kidney donation vs recipients of kidneys from deceased donors who did not undergo dialysis.
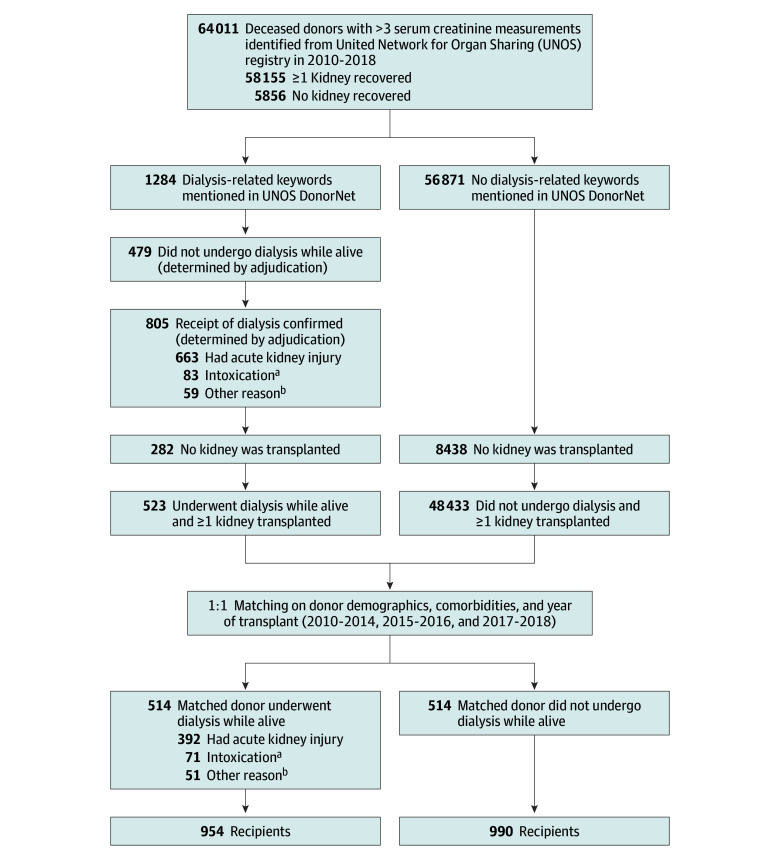
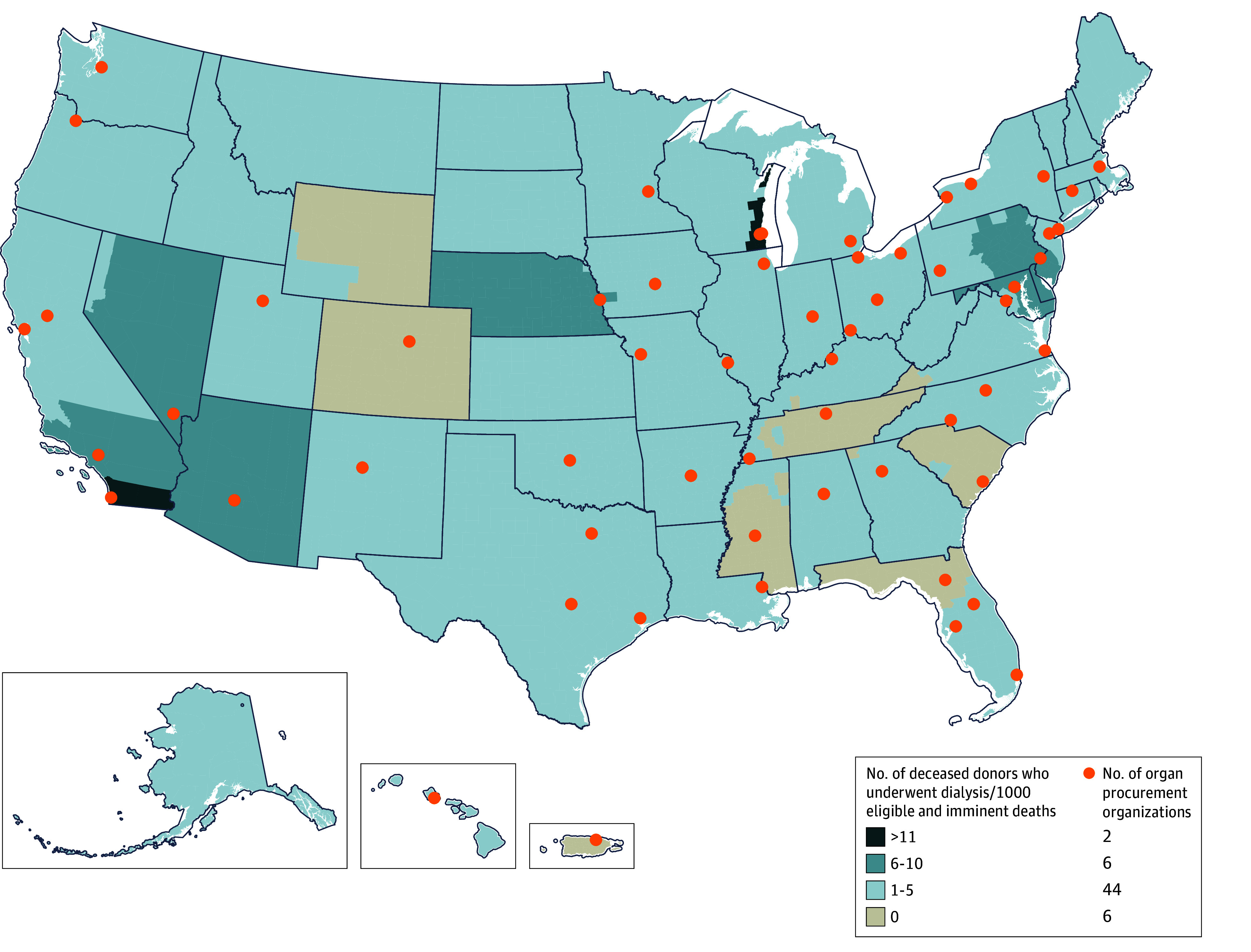
Design, setting, and participants: A retrospective cohort study was conducted including data from 58 US organ procurement organizations on deceased kidney donors and kidney transplant recipients. From 2010 to 2018, 805 donors who underwent dialysis prior to kidney donation were identified. The donors who underwent dialysis prior to kidney donation were matched 1:1 with donors who did not undergo dialysis using a rank-based distance matrix algorithm; 1944 kidney transplant recipients were evaluated.
Exposure: Kidney transplants from deceased donors who underwent dialysis prior to kidney donation compared with kidney transplants from deceased donors who did not undergo dialysis.
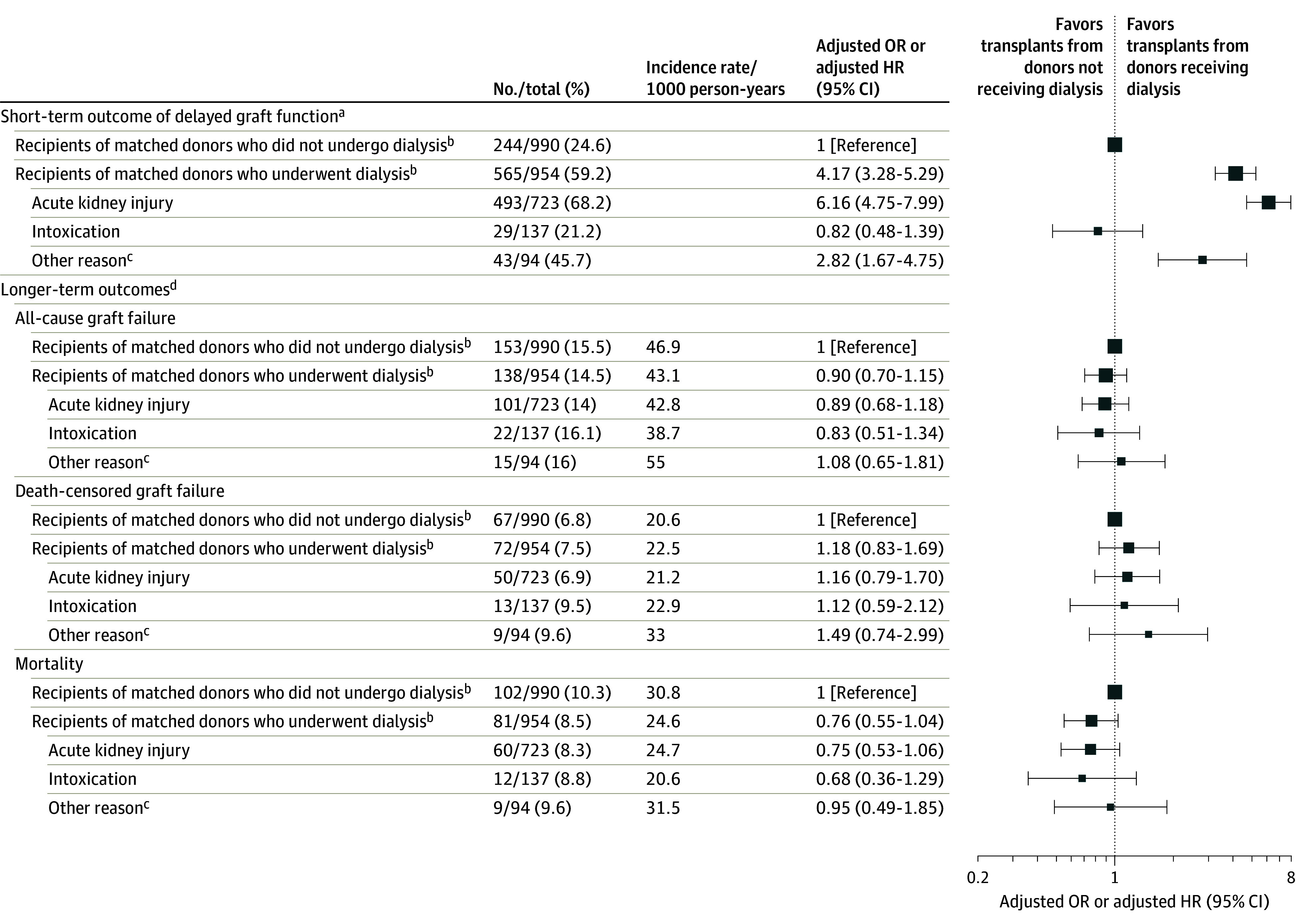
Main outcomes and measures: The 4 study outcomes were delayed graft function (defined as receipt of dialysis by the kidney recipient ≤1 week after transplant), all-cause graft failure, death-censored graft failure, and death.
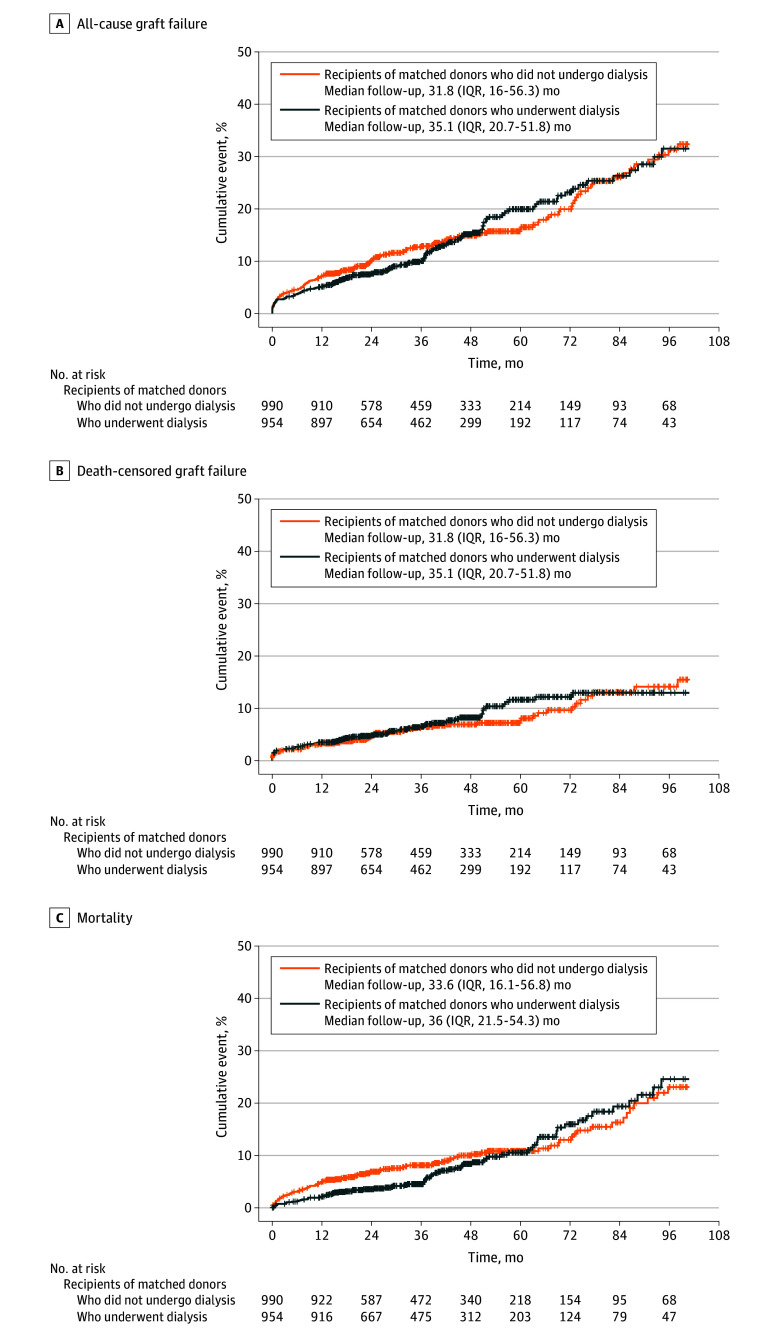
Results: From 2010 to 2018, 1.4% of deceased kidney donors (805 of 58 155) underwent dialysis prior to kidney donation. Of these 805 individuals, 523 (65%) donated at least 1 kidney. A total of 969 kidneys (60%) were transplanted and 641 kidneys (40%) were discarded. Among the donors with kidneys transplanted, 514 (mean age, 33 years [SD, 10.8 years]; 98 had hypertension [19.1%] and 36 had diabetes [7%]) underwent dialysis prior to donation and were matched with 514 (mean age, 33 years [SD, 10.9 years]; 98 had hypertension [19.1%] and 36 had diabetes [7%]) who did not undergo dialysis. Kidney transplants from donors who received dialysis prior to donation (n = 954 kidney recipients) were associated with a higher risk of delayed graft function compared with kidney transplants from donors who did not receive dialysis (n = 990 kidney recipients) (59.2% vs 24.6%, respectively; adjusted odds ratio, 4.17 [95% CI, 3.28-5.29]). The incidence rates did not significantly differ at a median follow-up of 34.1 months for all-cause graft failure (43.1 kidney transplants per 1000 person-years from donors who received dialysis prior to donation vs 46.9 kidney transplants per 1000 person-years from donors who did not receive dialysis; adjusted hazard ratio [HR], 0.90 [95% CI, 0.70-1.15]), for death-censored graft failure (22.5 vs 20.6 per 1000 person-years, respectively; adjusted HR, 1.18 [95% CI, 0.83-1.69]), or for death (24.6 vs 30.8 per 1000 person-years; adjusted HR, 0.76 [95% CI, 0.55-1.04]).
Conclusions and relevance: Compared with receiving a kidney from a deceased donor who did not undergo dialysis, receiving a kidney from a deceased donor who underwent dialysis prior to kidney donation was associated with a significantly higher incidence of delayed graft function, but no significant difference in graft failure or death at follow-up.
Conflict of interest statement
Figures
Comment in
-
Expanding the Overton Window in Deceased Kidney Donor Eligibility-Enough to Make a Difference?JAMA. 2024 Jul 16;332(3):199-200. doi: 10.1001/jama.2024.8734. JAMA. 2024. PMID: 38780501 No abstract available.
References
-
- US Department of Health and Human Services . OPTN/SRTR 2020 annual data report. Accessed May 6, 2024. https://srtr.transplant.hrsa.gov/annual_reports/2020_ADR_Preview.aspx
-
- US Department of Health and Human Services . OPTN: national data. Accessed January 18, 2022. https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/
Publication types
MeSH terms
Grants and funding
- R01 DK093770/DK/NIDDK NIH HHS/United States
- U01 DK116097/DK/NIDDK NIH HHS/United States
- K24 AI146137/AI/NIAID NIH HHS/United States
- U01 DK116066/DK/NIDDK NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- P30 DK079310/DK/NIDDK NIH HHS/United States
- R01 MD014161/MD/NIMHD NIH HHS/United States
- K23 DK127154/DK/NIDDK NIH HHS/United States
- T32 DK007732/DK/NIDDK NIH HHS/United States
- U01 DK126654/DK/NIDDK NIH HHS/United States
- R01 DK126739/DK/NIDDK NIH HHS/United States
- U01 DK110961/DK/NIDDK NIH HHS/United States
- U01 DK130058/DK/NIDDK NIH HHS/United States
- K24 DK090203/DK/NIDDK NIH HHS/United States
- R01 EB032910/EB/NIBIB NIH HHS/United States
- R01 DK123041/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
