

Are medical history data fit for risk stratification of patients with chest pain in emergency care? Comparing data collected from patients using computerized history taking with data documented by physicians in the electronic health record in the CLEOS-CPDS prospective cohort study
- PMID: 38781350
- PMCID: PMC11187423
- DOI: 10.1093/jamia/ocae110
Are medical history data fit for risk stratification of patients with chest pain in emergency care? Comparing data collected from patients using computerized history taking with data documented by physicians in the electronic health record in the CLEOS-CPDS prospective cohort study
Erratum in
-
Correction to: Are medical history data fit for risk stratification of patients with chest pain in emergency care? Comparing data collected from patients using computerized history taking with data documented by physicians in the electronic health record in the CLEOS-CPDS prospective cohort study.J Am Med Inform Assoc. 2025 Jan 1;32(1):261-263. doi: 10.1093/jamia/ocae252. J Am Med Inform Assoc. 2025. PMID: 39340474 Free PMC article. No abstract available.
Abstract
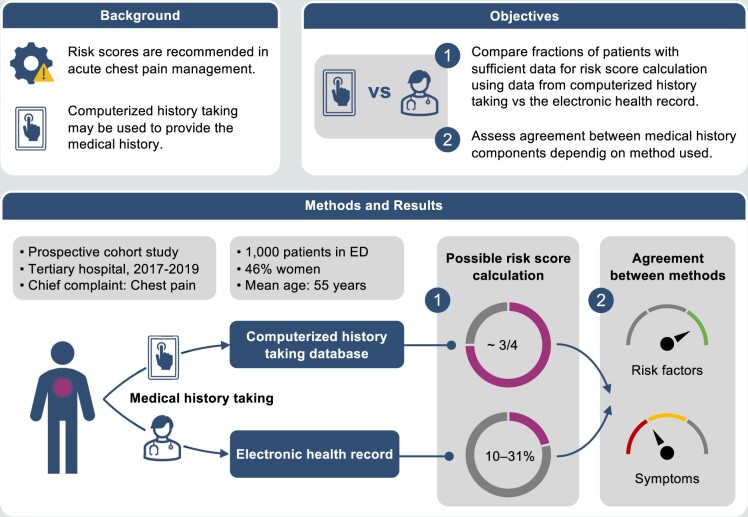
Objective: In acute chest pain management, risk stratification tools, including medical history, are recommended. We compared the fraction of patients with sufficient clinical data obtained using computerized history taking software (CHT) versus physician-acquired medical history to calculate established risk scores and assessed the patient-by-patient agreement between these 2 ways of obtaining medical history information.
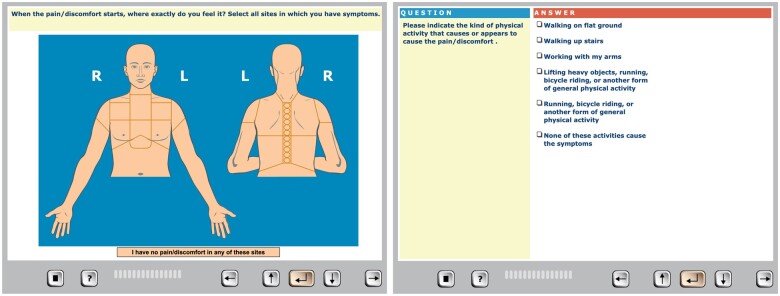
Materials and methods: This was a prospective cohort study of clinically stable patients aged ≥ 18 years presenting to the emergency department (ED) at Danderyd University Hospital (Stockholm, Sweden) in 2017-2019 with acute chest pain and non-diagnostic ECG and serum markers. Medical histories were self-reported using CHT on a tablet. Observations on discrete variables in the risk scores were extracted from electronic health records (EHR) and the CHT database. The patient-by-patient agreement was described by Cohen's kappa statistics.
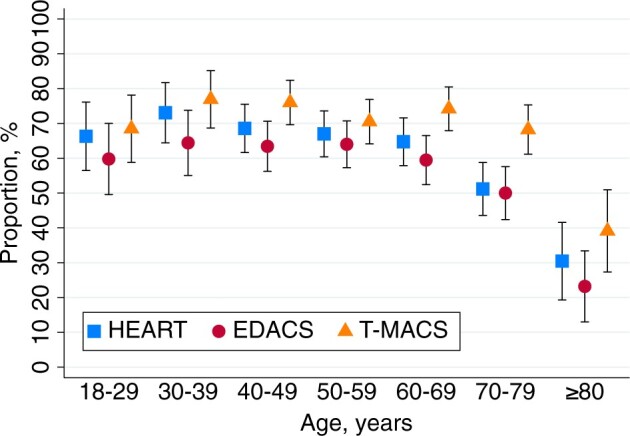
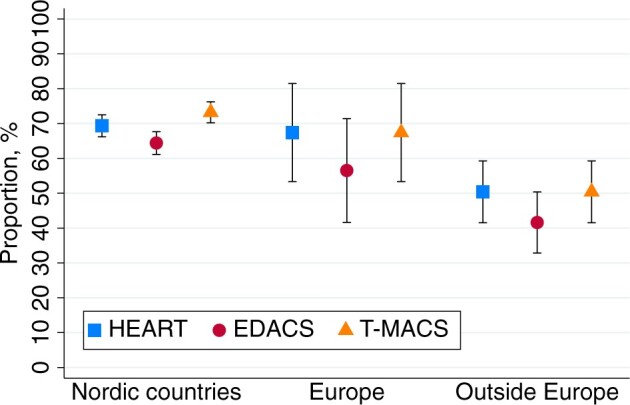
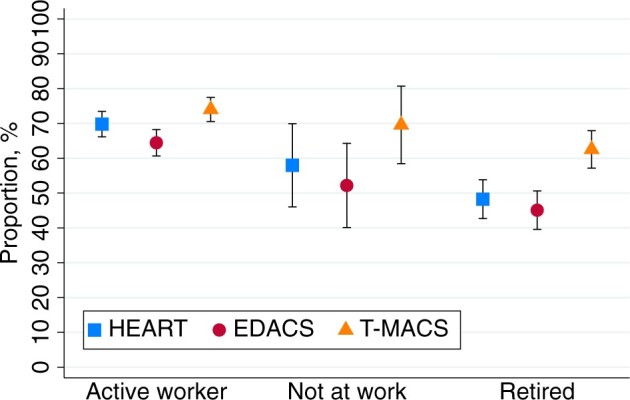
Results: Of the total 1000 patients included (mean age 55.3 ± 17.4 years; 54% women), HEART score, EDACS, and T-MACS could be calculated in 75%, 74%, and 83% by CHT and in 31%, 7%, and 25% by EHR, respectively. The agreement between CHT and EHR was slight to moderate (kappa 0.19-0.70) for chest pain characteristics and moderate to almost perfect (kappa 0.55-0.91) for risk factors.
Conclusions: CHT can acquire and document data for chest pain risk stratification in most ED patients using established risk scores, achieving this goal for a substantially larger number of patients, as compared to EHR data. The agreement between CHT and physician-acquired history taking is high for traditional risk factors and lower for chest pain characteristics.
Clinical trial registration: ClinicalTrials.gov NCT03439449.
Keywords: acute coronary syndrome; artificial intelligence; chest pain; medical history taking; medical informatics.
© The Author(s) 2024. Published by Oxford University Press on behalf of the American Medical Informatics Association.
Conflict of interest statement
All patent rights and copyrights to technology, language, images, and knowledge content are assigned without royalty rights to Karolinska Institutet, Stockholm, Sweden, which is a public university. T.K.: Research grants to Karolinska Institutet from Medtronic, and ReCor Medical; all outside the submitted work. J.S.: Speaker honoraria for AstraZeneca, Bayer, NovoNordisk, and Medtronic, and shareholder in Beat Vascular Health. No conflicts of interests to declare by H.B., S.K., or C.J.S.
Figures
Similar articles
-
A prospective cohort study of self-reported computerised medical history taking for acute chest pain: protocol of the CLEOS-Chest Pain Danderyd Study (CLEOS-CPDS).BMJ Open. 2020 Jan 21;10(1):e031871. doi: 10.1136/bmjopen-2019-031871. BMJ Open. 2020. PMID: 31969363 Free PMC article.
-
Use of Self-Reported Computerized Medical History Taking for Acute Chest Pain in the Emergency Department - the Clinical Expert Operating System Chest Pain Danderyd Study (CLEOS-CPDS): Prospective Cohort Study.J Med Internet Res. 2021 Apr 27;23(4):e25493. doi: 10.2196/25493. J Med Internet Res. 2021. PMID: 33904821 Free PMC article.
-
Computerized history-taking improves data quality for clinical decision-making-Comparison of EHR and computer-acquired history data in patients with chest pain.PLoS One. 2021 Sep 27;16(9):e0257677. doi: 10.1371/journal.pone.0257677. eCollection 2021. PLoS One. 2021. PMID: 34570811 Free PMC article.
-
Applications of machine learning to undifferentiated chest pain in the emergency department: A systematic review.PLoS One. 2021 Aug 24;16(8):e0252612. doi: 10.1371/journal.pone.0252612. eCollection 2021. PLoS One. 2021. PMID: 34428208 Free PMC article.
-
HEART Score Risk Stratification of Low-Risk Chest Pain Patients in the Emergency Department: A Systematic Review and Meta-Analysis.Ann Emerg Med. 2019 Aug;74(2):187-203. doi: 10.1016/j.annemergmed.2018.12.010. Epub 2019 Feb 2. Ann Emerg Med. 2019. PMID: 30718010
Cited by
-
Predicting the risk of postoperative gastrointestinal bleeding in patients with Type A aortic dissection based on an interpretable machine learning model.Front Med (Lausanne). 2025 May 19;12:1554579. doi: 10.3389/fmed.2025.1554579. eCollection 2025. Front Med (Lausanne). 2025. PMID: 40458646 Free PMC article.
-
Performance of computerized self-reported medical history taking and HEAR score for safe early rule-out of cardiac events in acute chest pain patients: the CLEOS-CPDS prospective cohort study.Eur Heart J Digit Health. 2024 Nov 12;6(1):104-114. doi: 10.1093/ehjdh/ztae087. eCollection 2025 Jan. Eur Heart J Digit Health. 2024. PMID: 39846077 Free PMC article.
-
Patient Perspectives on Digital Technology and Experiences of Computerized History-Taking for Chest Pain Management in the Emergency Department: CLEOS-CPDS Prospective Cohort Study.JMIR Med Inform. 2025 Jun 17;13:e65568. doi: 10.2196/65568. JMIR Med Inform. 2025. PMID: 40526888 Free PMC article.
References
-
- Bjornsen LP, Naess-Pleym LE, Dale J, et al. Description of chest pain patients in a Norwegian emergency department. Scand Cardiovasc J. 2019;53(1):28-34. - PubMed
-
- Martinez-Selles M, Bueno H, Sacristan A, et al. Chest pain in the emergency department: incidence, clinical characteristics and risk stratification. Rev Esp Cardiol. 2008;61(9):953-959. - PubMed
-
- Byrne RA, Rossello X, Coughlan JJ, ESC Scientific Document Group, et al. 2023 ESC Guidelines for the management of acute coronary syndromes. Eur Heart J. 2023;44(38):3720-3826. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
