

Cisternal and intraventricular irrigation in subarachnoid and intraventricular haemorrhage
- PMID: 38782496
- PMCID: PMC11877441
- DOI: 10.1136/svn-2023-003062
Cisternal and intraventricular irrigation in subarachnoid and intraventricular haemorrhage
Abstract
Background: Subarachnoid haemorrhage (SAH) and intraventricular haemorrhage (IVH) are associated with poor patient outcomes. Intraventricular fibrinolysis is effective in clearing IVH and improving patient survival and neurological outcome. By similar rationale, cisternal irrigation has been proposed as a potential method to accelerate haematoma clearance in SAH. We aimed to provide a comprehensive review and meta-analysis evaluating the effect of intraventricular and cisternal irrigation on clinical outcomes in patients with SAH and IVH.
Methods: The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed preparing this systematic review and study selection was performed by multiple investigators. We extracted ORs from the individual studies and aggregated these using a random effects model. The quality of evidence was evaluated using Grading of Recommendations, Assessment, Development and Evaluations assessment and ROBINS-I or RoB-2.
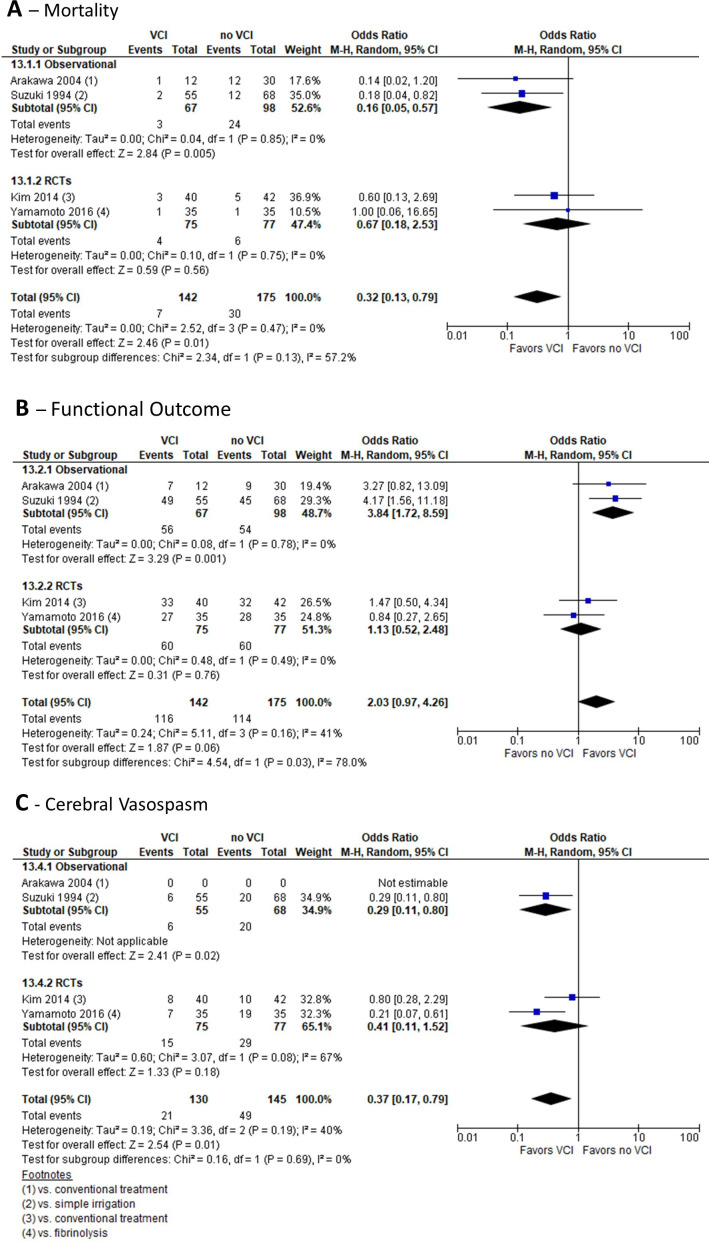
Results: 24 articles were included. In SAH, we found that cisternal irrigation with fibrinolytic agents was associated with reduced mortality (OR: 0.68, 95% CI 0.46 to 1.00), higher probability of favourable functional outcome (OR: 1.80, 95% CI 1.30 to 2.51), and reduced risks of DCI (OR: 0.28, 95% CI 0.18 to 0.42) and cerebral vasospasm (OR: 0.28, 95% CI 0.18 to 0.42), compared with conventional therapy. Cisternal irrigation with vasodilatory agents was associated with lower mortality (OR: 0.32, 95% CI 0.13 to 0.79) and reduced risk of cerebral vasospasm (OR: 0.37, 95% CI 0.17 to 0.79). The evidence for irrigation therapy of IVH was sparse and insufficient to show any significant effect.
Conclusion: In this study, we found that cisternal irrigation could improve the prognosis in patients with SAH compared with conventional therapy. There is no evidence to support cisternal irrigation treatment of IVH.
Keywords: Hemorrhage; Intracranial Aneurysm; Subarachnoid.
© Author(s) (or their employer(s)) 2025. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ Group.
Conflict of interest statement
Competing interests: ARK reports grants from IRRAS AB to Aarhus University Hospital to support the ACTIVE study and personal fees from IRRAS AB for a presentation at a scientific symposium describing his experiences with the IRRAflow technology during the conduct of the study; grants from IRRAS AB to Aarhus University Hos-pital to support the development of a neuromonitoring technology related to IRRAflow outside the submitted work; in addition, ARK has a patent for a neuromonitoring technology pending with relation to the IRRAflow technology. The remaining authors have no conflicts of interest to declare.
Figures



References
-
- Coppadoro A, Citerio G. Subarachnoid hemorrhage: an update for the Intensivist. Minerva Anestesiol. 2011;77:74–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources