

Dose escalation study of a personalized peptide-based neoantigen vaccine (EVX-01) in patients with metastatic melanoma
- PMID: 38782542
- PMCID: PMC11116868
- DOI: 10.1136/jitc-2024-008817
Dose escalation study of a personalized peptide-based neoantigen vaccine (EVX-01) in patients with metastatic melanoma
Abstract
Background: Neoantigens can serve as targets for T cell-mediated antitumor immunity via personalized neopeptide vaccines. Interim data from our clinical study NCT03715985 showed that the personalized peptide-based neoantigen vaccine EVX-01, formulated in the liposomal adjuvant, CAF09b, was safe and able to elicit EVX-01-specific T cell responses in patients with metastatic melanoma. Here, we present results from the dose-escalation part of the study, evaluating the feasibility, safety, efficacy, and immunogenicity of EVX-01 in addition to anti-PD-1 therapy.
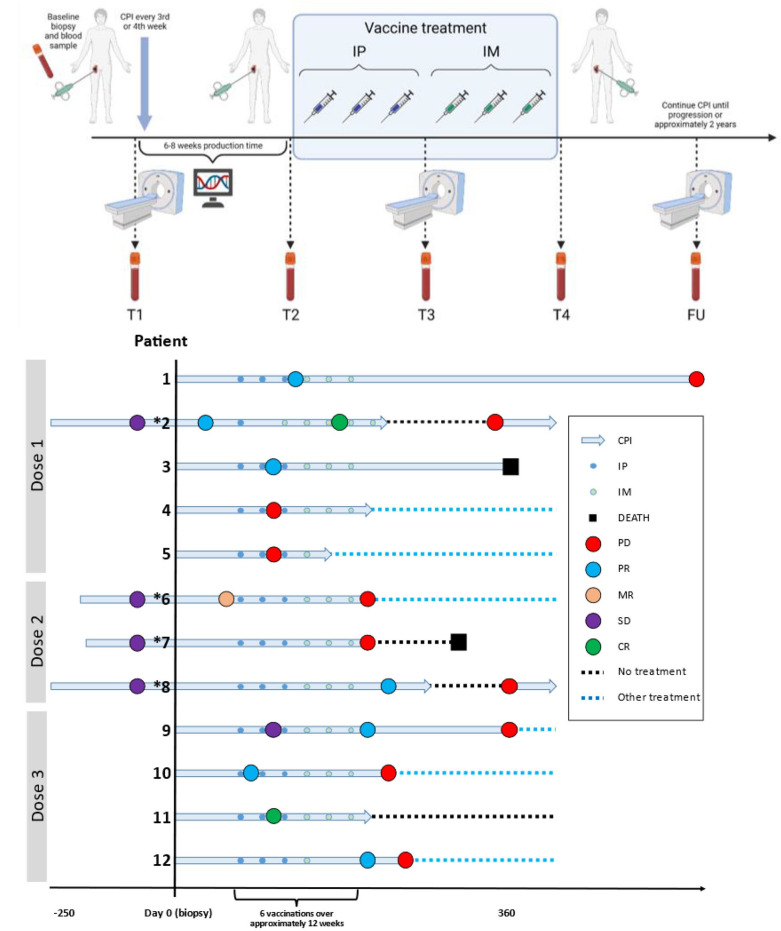
Methods: Patients with metastatic melanoma on anti-PD-1 therapy were treated in three cohorts with increasing vaccine dosages (twofold and fourfold). Tumor-derived neoantigens were selected by the AI platform PIONEER and used in personalized therapeutic cancer peptide vaccines EVX-01. Vaccines were administered at 2-week intervals for a total of three intraperitoneal and three intramuscular injections. The study's primary endpoint was safety and tolerability. Additional endpoints were immunological responses, survival, and objective response rates.
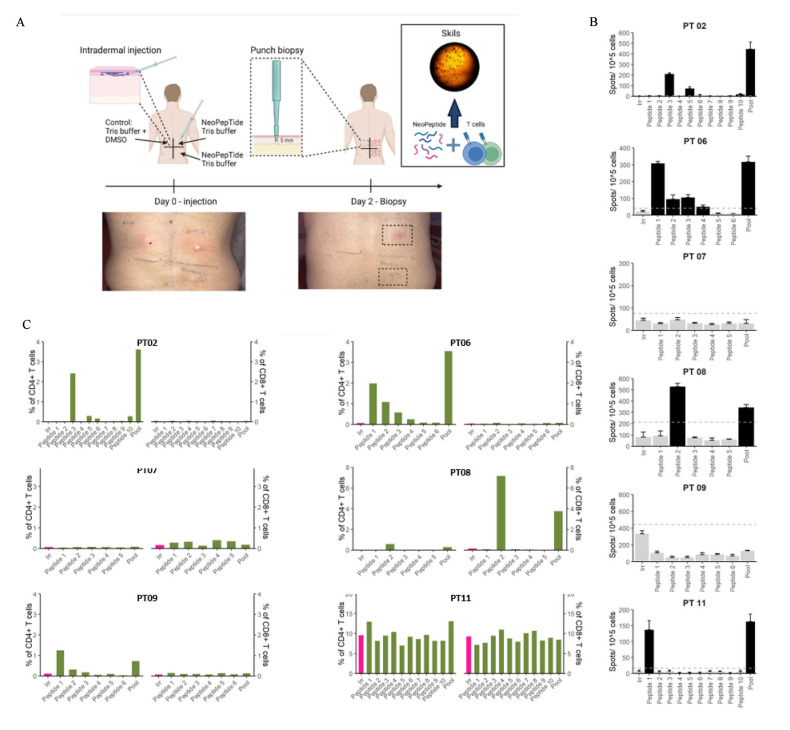
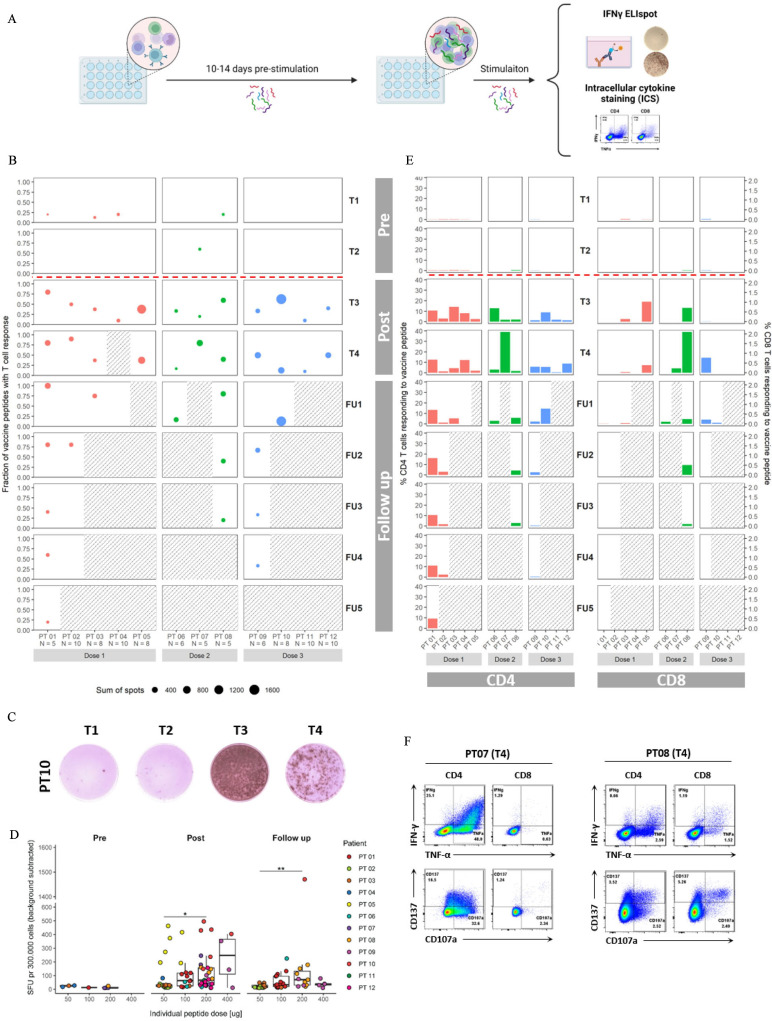
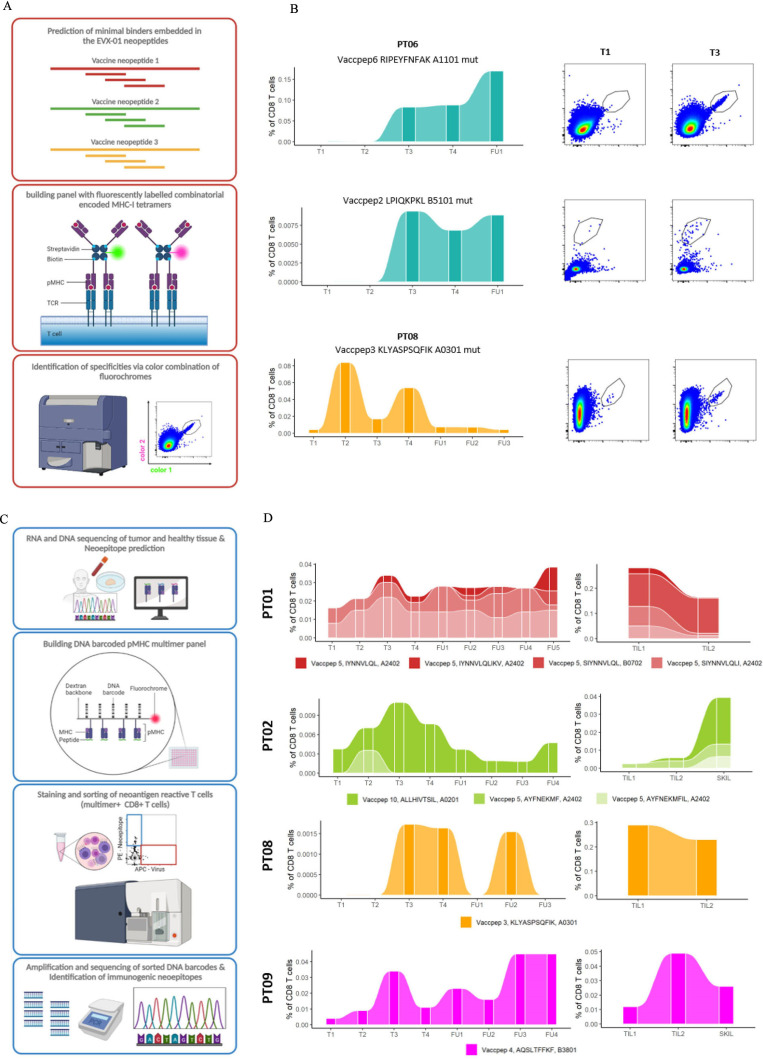
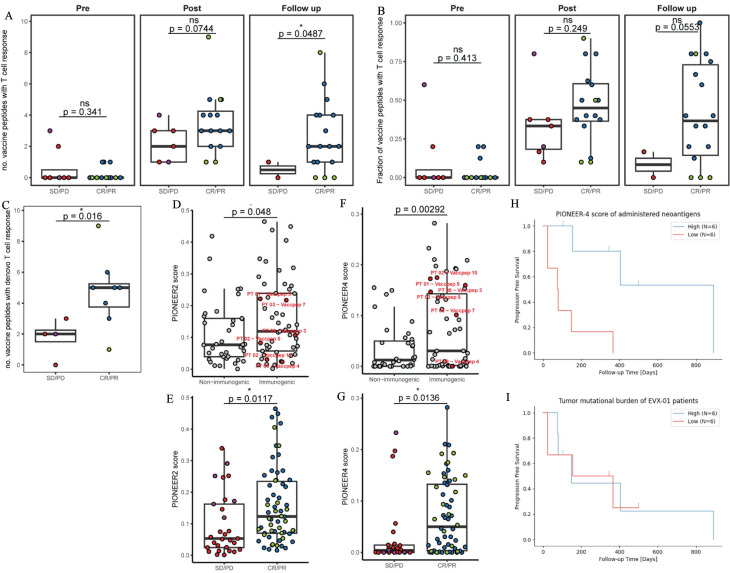
Results: Compared with the base dose level previously reported, no new vaccine-related serious adverse events were observed during dose escalation of EVX-01 in combination with an anti-PD-1 agent given according to local guidelines. Two patients at the third dose level (fourfold dose) developed grade 3 toxicity, most likely related to pembrolizumab. Overall, 8 out of the 12 patients had objective clinical responses (6 partial response (PR) and 2 CR), with all 4 patients at the highest dose level having a CR (1 CR, 3 PR). EVX-01 induced peptide-specific CD4+ and/or CD8+T cell responses in all treated patients, with CD4+T cells as the dominating responses. The magnitude of immune responses measured by IFN-γ ELISpot assay correlated with individual peptide doses. A significant correlation between the PIONEER quality score and induced T cell immunogenicity was detected, while better CRs correlated with both the number of immunogenic EVX-01 peptides and the PIONEER quality score.
Conclusion: Immunization with EVX-01-CAF09b in addition to anti-PD-1 therapy was shown to be safe and well tolerated and elicit vaccine neoantigen-specific CD4+and CD8+ T cell responses at all dose levels. In addition, objective tumor responses were observed in 67% of patients. The results encourage further assessment of the antitumor efficacy of EVX-01 in combination with anti-PD-1 therapy.
Keywords: immunotherapy; vaccine.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY-NC. No commercial re-use. See rights and permissions. Published by BMJ.
Conflict of interest statement
Competing interests: MD has received honoraria for lectures from Roche and Novartis (past 2 years). IMS has received honoraria for lectures and consultancies from Novartis, Roche, MSD, BMS, and Pierre Fabre. KB has received honoraria (institutional) for lectures and advisory boards of MSD, Pierre Fabre, and BMS. CCIT-DK has been granted economic support for personal wages from Evaxion Biotech A/S, Denmark. SRH is a cofounder of PokeACell and coinventor of several licensed patents. ABS, DK-K, AJ, NVP, NT and JK are employees of Evaxion Biotech A/S and have a financial interest in the company. All other authors have declared that they have no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
Research Materials