

Metabolic pathway-based subtypes associate glycan biosynthesis and treatment response in head and neck cancer
- PMID: 38783045
- PMCID: PMC11116554
- DOI: 10.1038/s41698-024-00602-0
Metabolic pathway-based subtypes associate glycan biosynthesis and treatment response in head and neck cancer
Abstract
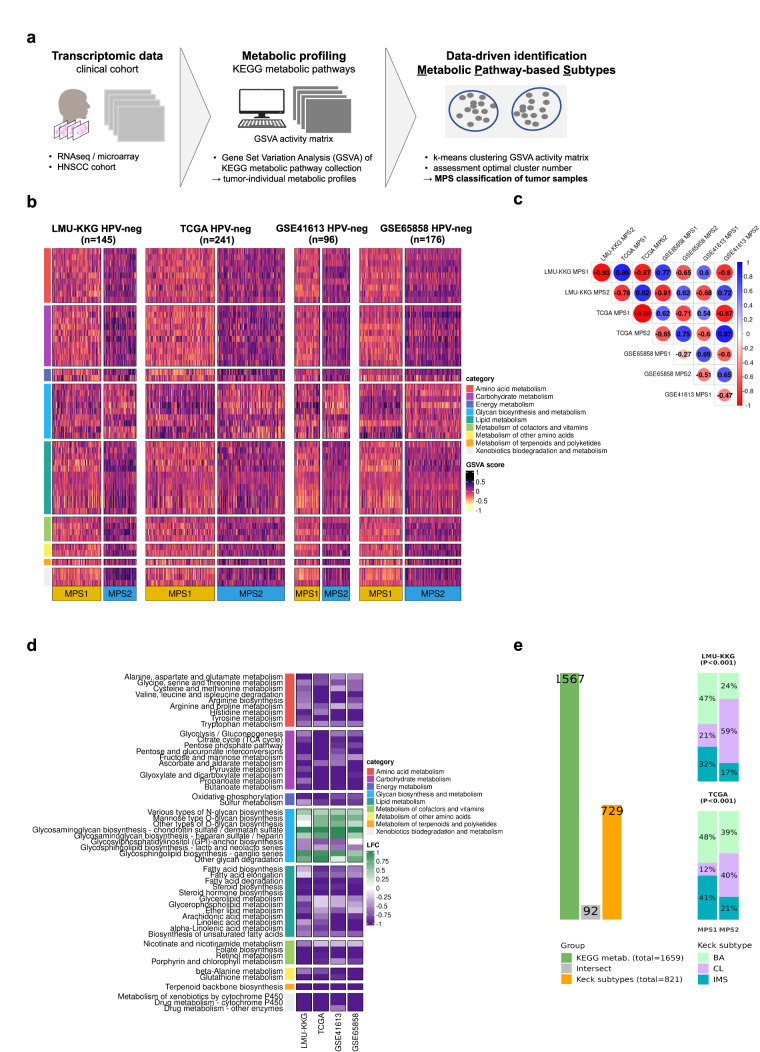
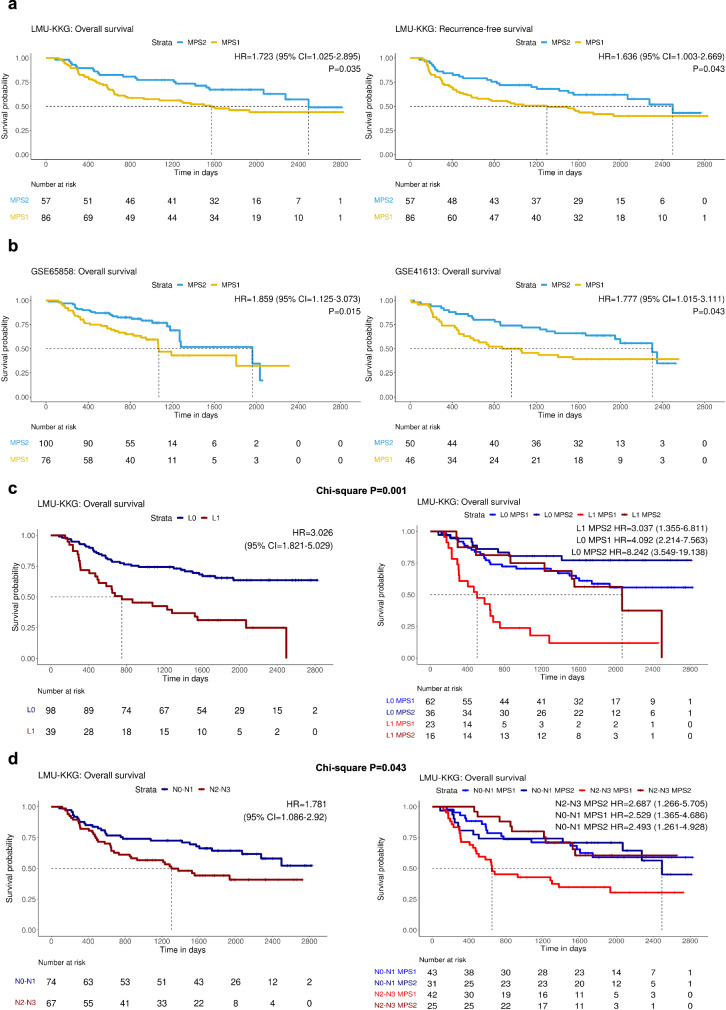
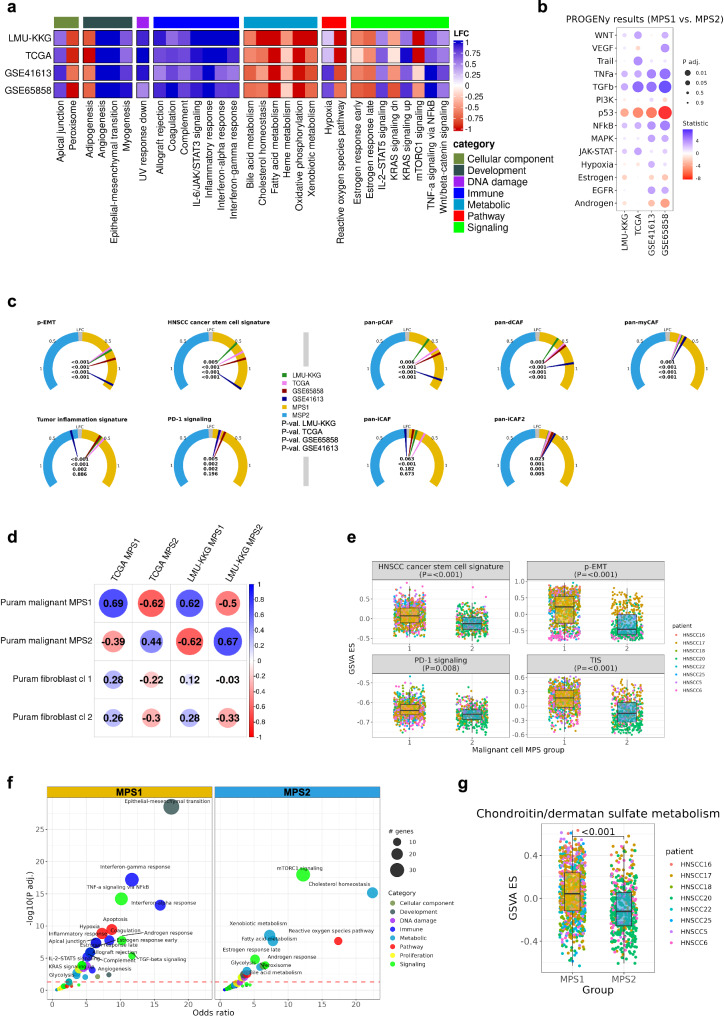
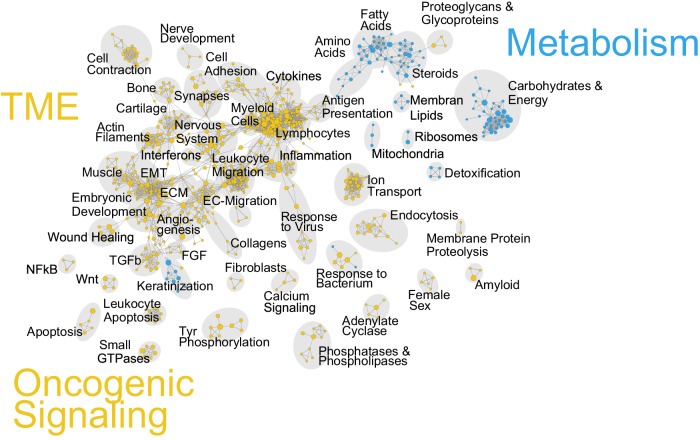
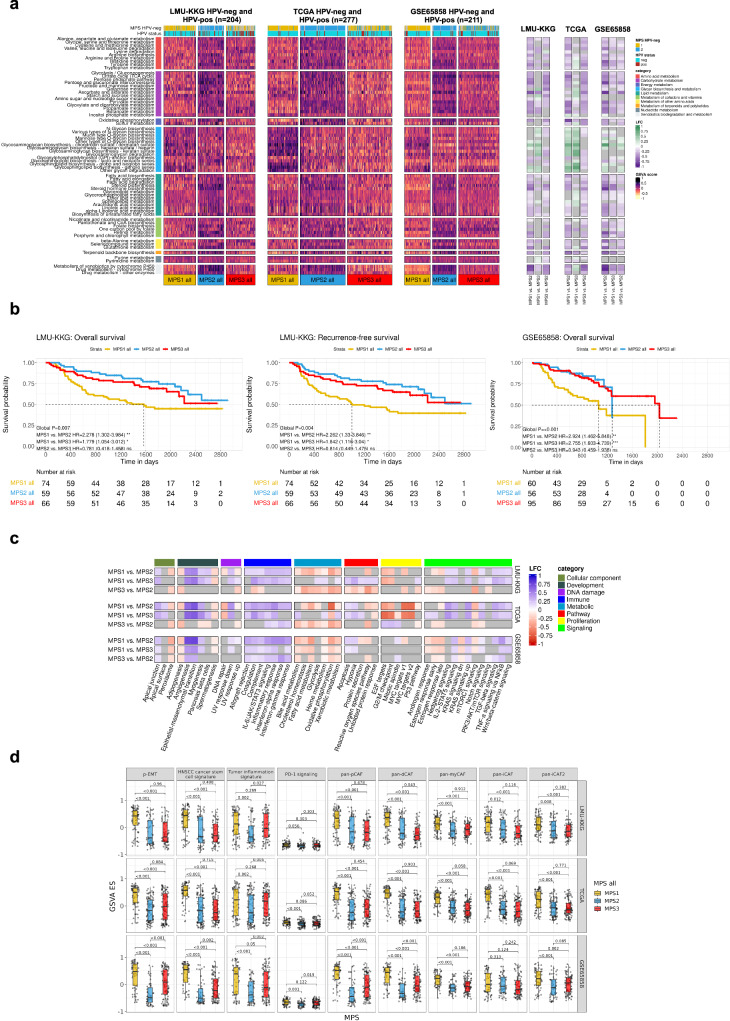
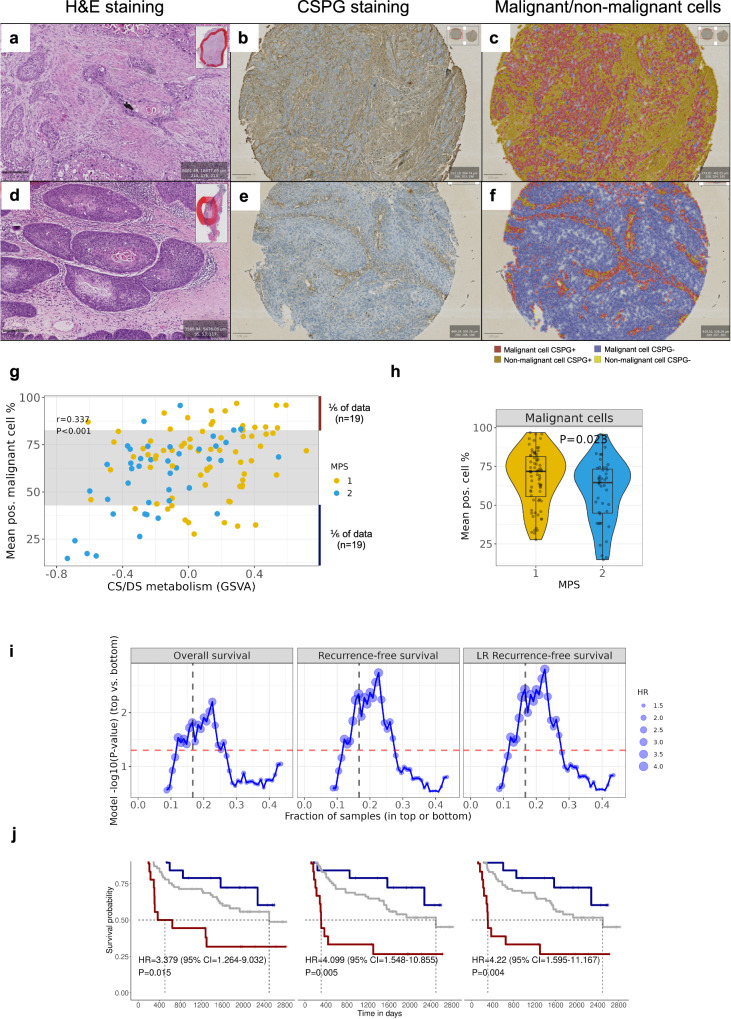
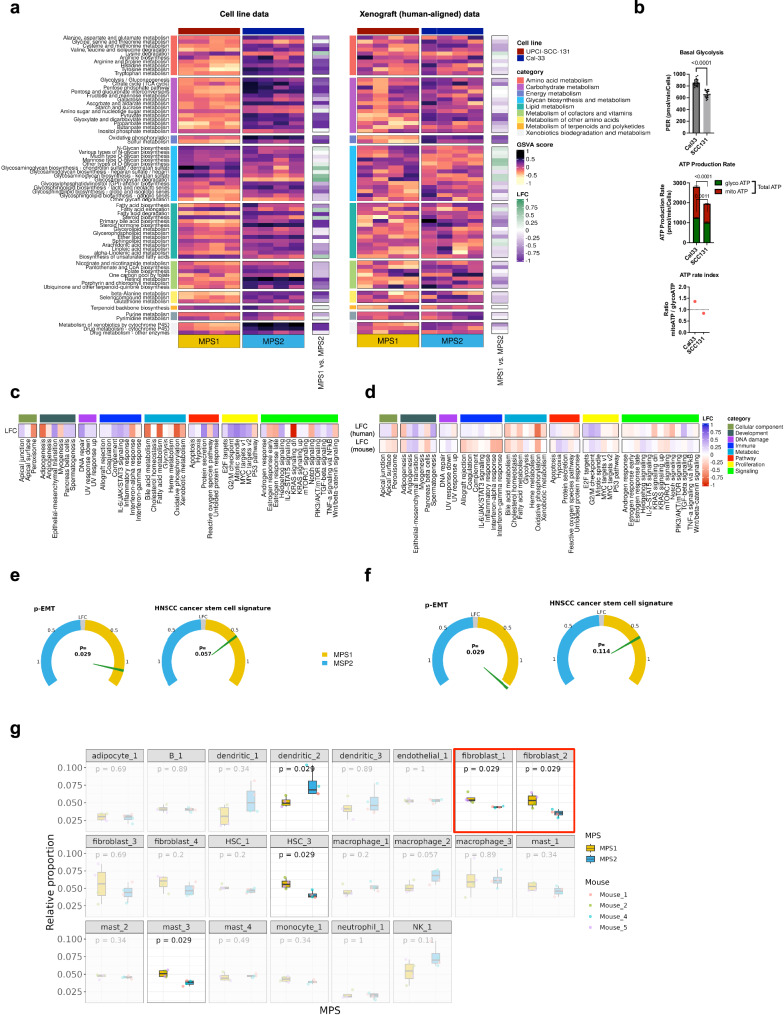
Head and Neck Squamous Cell Carcinoma (HNSCC) is a heterogeneous malignancy that remains a significant challenge in clinical management due to frequent treatment failures and pronounced therapy resistance. While metabolic dysregulation appears to be a critical factor in this scenario, comprehensive analyses of the metabolic HNSCC landscape and its impact on clinical outcomes are lacking. This study utilized transcriptomic data from four independent clinical cohorts to investigate metabolic heterogeneity in HNSCC and define metabolic pathway-based subtypes (MPS). In HPV-negative HNSCCs, MPS1 and MPS2 were identified, while MPS3 was enriched in HPV-positive cases. MPS classification was associated with clinical outcome post adjuvant radio(chemo)therapy, with MPS1 consistently exhibiting the highest risk of therapeutic failure. MPS1 was uniquely characterized by upregulation of glycan (particularly chondroitin/dermatan sulfate) metabolism genes. Immunohistochemistry and pilot mass spectrometry imaging analyses confirmed this at metabolite level. The histological context and single-cell RNA sequencing data identified the malignant cells as key contributors. Globally, MPS1 was distinguished by a unique transcriptomic landscape associated with increased disease aggressiveness, featuring motifs related to epithelial-mesenchymal transition, immune signaling, cancer stemness, tumor microenvironment assembly, and oncogenic signaling. This translated into a distinct histological appearance marked by extensive extracellular matrix remodeling, abundant spindle-shaped cancer-associated fibroblasts, and intimately intertwined populations of malignant and stromal cells. Proof-of-concept data from orthotopic xenotransplants replicated the MPS phenotypes on the histological and transcriptome levels. In summary, this study introduces a metabolic pathway-based classification of HNSCC, pinpointing glycan metabolism-enriched MPS1 as the most challenging subgroup that necessitates alternative therapeutic strategies.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
