

Correlation and risk factors of peripheral and cervicocephalic arterial atherosclerosis in patients with ischemic cerebrovascular disease
- PMID: 38783071
- PMCID: PMC11116411
- DOI: 10.1038/s41598-024-62092-1
Correlation and risk factors of peripheral and cervicocephalic arterial atherosclerosis in patients with ischemic cerebrovascular disease
Abstract
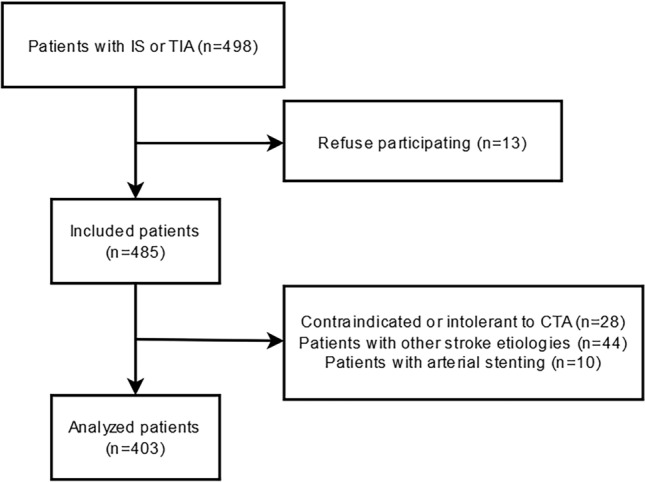
Patients with ischemic cerebrovascular disease (ICVD) frequently develop concomitant peripheral artery disease (PAD) or renal artery stenosis (RAS), and multiterritorial atherosclerotic patients usually have a worse prognosis. We aimed to evaluate the status of peripheral atherosclerosis (AS) and cervicocephalic AS (CAS) in ICVD patients with AS, their correlation, and related risk factors contributing to coexisting cervicocephalic-peripheral AS (CPAS). Based on the severity and extent of AS evaluated by computed tomography angiography and ultrasound, the degree of AS was triple categorized to assess the correlation between CAS and PAD/RAS. CAS and PAD/RAS were defined as the most severe stenosis being ≥ 50% luminal diameter in cervicocephalic or lower limb arteries, and a peak systolic velocity at the turbulent site being ≥ 180 cm/s in the renal artery. Among 403 patients with symptom onset within 30 days, CAS, PAD, and RAS occurrence rates were 68.7%, 25.3%, and 9.9%, respectively. PAD was independently associated with the degree of extracranial and intracranial CAS (p = 0.042, OR = 1.428, 95% CI 1.014-2.012; p = 0.002, OR = 1.680, 95% CI 1.206-2.339), while RAS was independently associated with the degree of extracranial CAS (p = 0.001, OR = 2.880, 95% CI 1.556-5.329). Independent CPAS risk factors included an ischemic stroke history (p = 0.033), increased age (p < 0.01), as well as elevated fibrinogen (p = 0.021) and D-dimer levels (p = 0.019). In conclusion, the occurrence rates of RAS and PAD in ICVD patients with AS is relatively high, and with the severity of RAS or PAD increase, the severity of CAS also increase. Strengthening the evaluation of peripheral AS and controlling elevated fibrinogen might be crucial for preventing and delaying the progression of multiterritorial AS in ICVD patients with AS, thereby improving risk stratification and promoting more effective prevention and treatment strategies.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
