

Utilizing machine learning to predict post-treatment outcomes in chronic non-specific neck pain patients undergoing cervical extension traction
- PMID: 38783089
- PMCID: PMC11116459
- DOI: 10.1038/s41598-024-62812-7
Utilizing machine learning to predict post-treatment outcomes in chronic non-specific neck pain patients undergoing cervical extension traction
Abstract
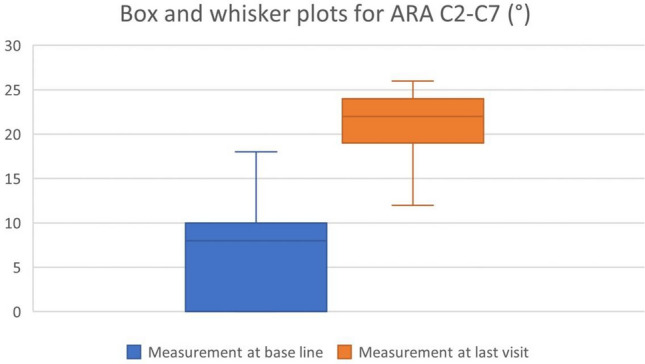
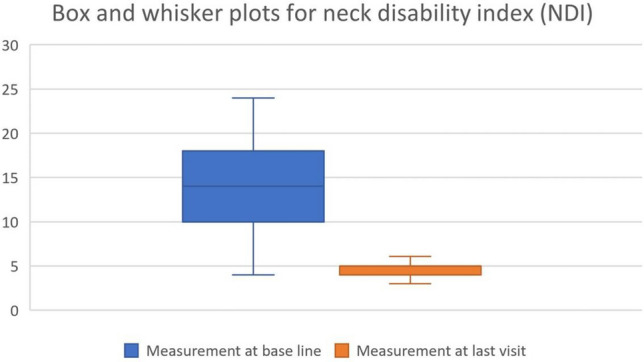
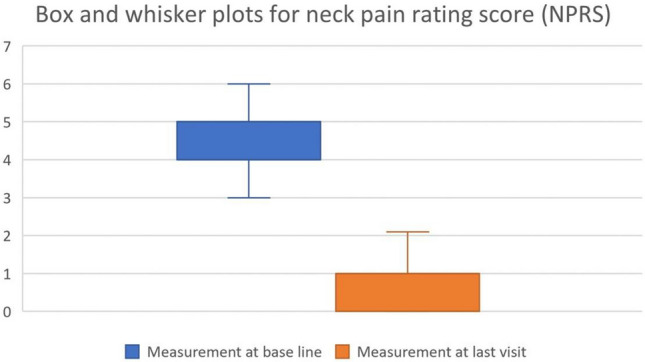
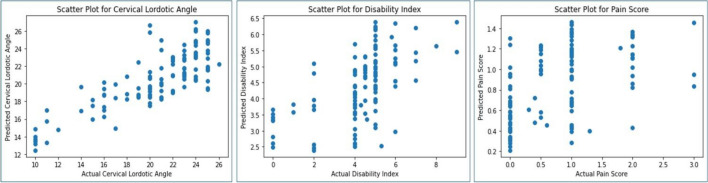
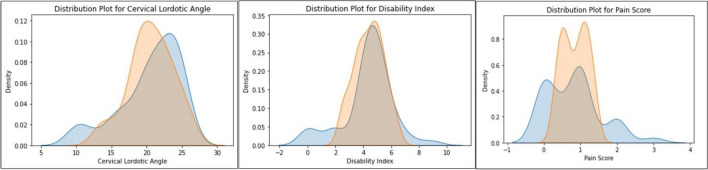
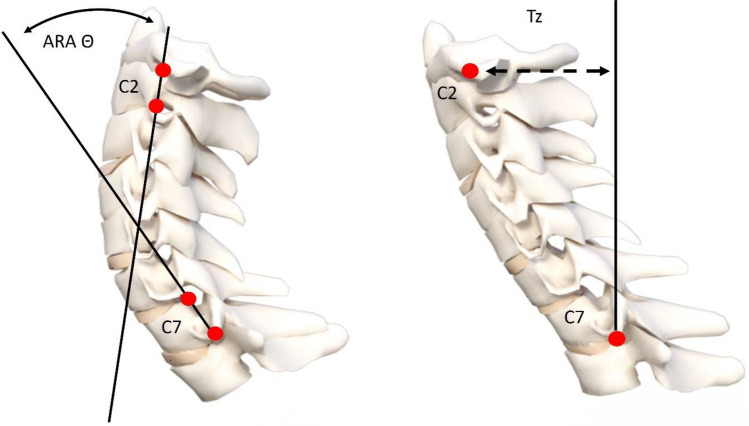
This study explored the application of machine learning in predicting post-treatment outcomes for chronic neck pain patients undergoing a multimodal program featuring cervical extension traction (CET). Pre-treatment demographic and clinical variables were used to develop predictive models capable of anticipating modifications in cervical lordotic angle (CLA), pain and disability of 570 patients treated between 2014 and 2020. Linear regression models used pre-treatment variables of age, body mass index, CLA, anterior head translation, disability index, pain score, treatment frequency, duration and compliance. These models used the sci-kit-learn machine learning library within Python for implementing linear regression algorithms. The linear regression models demonstrated high precision and accuracy, and effectively explained 30-55% of the variability in post-treatment outcomes, the highest for the CLA. This pioneering study integrates machine learning into spinal rehabilitation. The developed models offer valuable information to customize interventions, set realistic expectations, and optimize treatment strategies based on individual patient characteristics as treated conservatively with rehabilitation programs using CET as part of multimodal care.
Keywords: Cervical spine; Disability; Lordosis; Machine learning; Neck pain; Prediction; Traction.
© 2024. The Author(s).
Conflict of interest statement
PAO is a paid consultant for CBP NonProfit, Inc. DEH teaches rehabilitation methods and is the CEO of a company that distributes the DCTO product to physicians in the U.S.A. used in this manuscript. All the other authors declare that they have no competing interests.
Figures

Similar articles
-
The effect of normalizing the sagittal cervical configuration on dizziness, neck pain, and cervicocephalic kinesthetic sensibility: a 1-year randomized controlled study.Eur J Phys Rehabil Med. 2017 Feb;53(1):57-71. doi: 10.23736/S1973-9087.16.04179-4. Epub 2016 Aug 30. Eur J Phys Rehabil Med. 2017. PMID: 27575013 Clinical Trial.
-
Is Cervical Traction Effective in Chronic Nonspecific Neck Pain Patients With Unsatisfactory NSAID Control? A Nomogram to Predict Effectiveness.World Neurosurg. 2020 Jul;139:e245-e254. doi: 10.1016/j.wneu.2020.03.195. Epub 2020 Apr 11. World Neurosurg. 2020. PMID: 32289511
-
Development of a clinical prediction rule to identify patients with neck pain likely to benefit from cervical traction and exercise.Eur Spine J. 2009 Mar;18(3):382-91. doi: 10.1007/s00586-008-0859-7. Epub 2009 Jan 14. Eur Spine J. 2009. PMID: 19142674 Free PMC article.
-
Restoring cervical lordosis by cervical extension traction methods in the treatment of cervical spine disorders: a systematic review of controlled trials.J Phys Ther Sci. 2021 Oct;33(10):784-794. doi: 10.1589/jpts.33.784. Epub 2021 Oct 13. J Phys Ther Sci. 2021. PMID: 34658525 Free PMC article. Review.
-
Pediatric cervical kyphosis in the MRI era (1984-2008) with long-term follow up: literature review.Childs Nerv Syst. 2022 Feb;38(2):361-377. doi: 10.1007/s00381-021-05409-z. Epub 2021 Nov 22. Childs Nerv Syst. 2022. PMID: 34806157 Review.
Cited by
-
The magnitude of sagittal head posture displacement and patient demographics predict rehabilitation outcomes in patients with chronic nonspecific neck pain.Sci Rep. 2025 May 30;15(1):18986. doi: 10.1038/s41598-025-04187-x. Sci Rep. 2025. PMID: 40447787 Free PMC article.
-
Scoping Review of Machine Learning and Patient-Reported Outcomes in Spine Surgery.Bioengineering (Basel). 2025 Jan 29;12(2):125. doi: 10.3390/bioengineering12020125. Bioengineering (Basel). 2025. PMID: 40001645 Free PMC article. Review.
-
A comparative study on TB incidence and HIVTB coinfection using machine learning models on WHO global TB dataset.Sci Rep. 2025 Apr 21;15(1):13690. doi: 10.1038/s41598-025-94378-3. Sci Rep. 2025. PMID: 40258881 Free PMC article.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
