

Diabetes drugs activate neuroprotective pathways in models of neonatal hypoxic-ischemic encephalopathy
- PMID: 38783166
- PMCID: PMC11178908
- DOI: 10.1038/s44321-024-00079-1
Diabetes drugs activate neuroprotective pathways in models of neonatal hypoxic-ischemic encephalopathy
Abstract
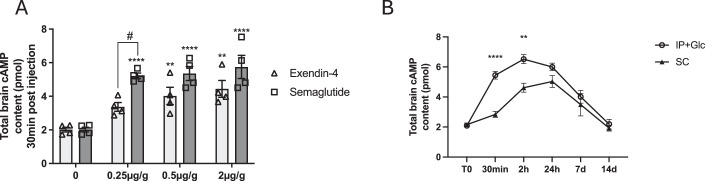
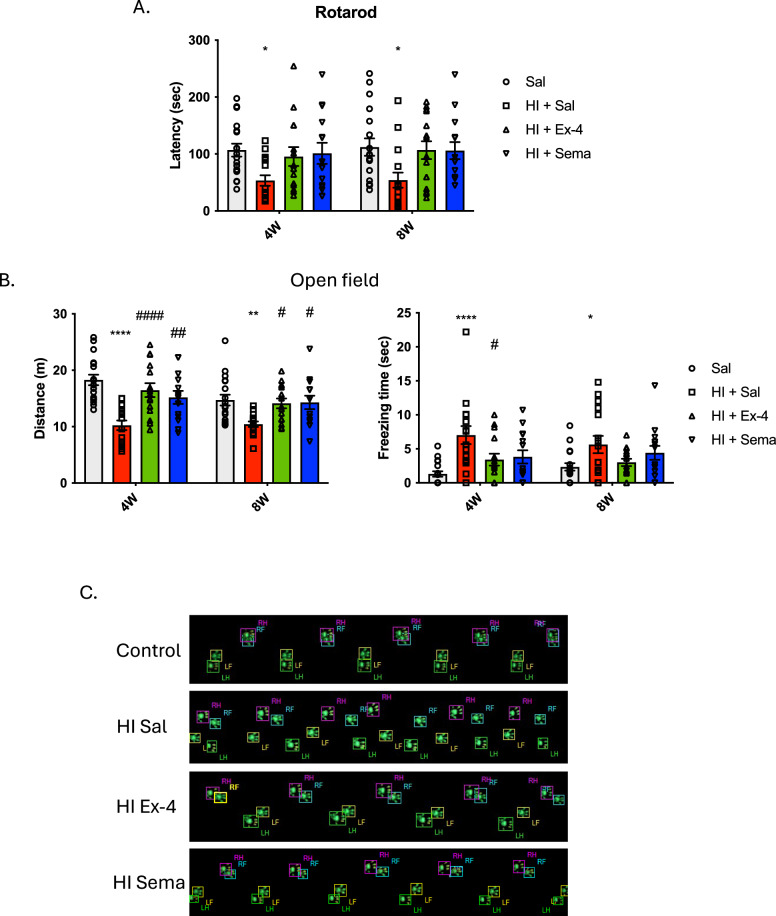
Hypoxic-ischaemic encephalopathy (HIE) arises from diminished blood flow and oxygen to the neonatal brain during labor, leading to infant mortality or severe brain damage, with a global incidence of 1.5 per 1000 live births. Glucagon-like Peptide 1 Receptor (GLP1-R) agonists, used in type 2 diabetes treatment, exhibit neuroprotective effects in various brain injury models, including HIE. In this study, we observed enhanced neurological outcomes in post-natal day 10 mice with surgically induced hypoxic-ischaemic (HI) brain injury after immediate systemic administration of exendin-4 or semaglutide. Short- and long-term assessments revealed improved neuropathology, survival rates, and locomotor function. We explored the mechanisms by which GLP1-R agonists trigger neuroprotection and reduce inflammation following oxygen-glucose deprivation and HI in neonatal mice, highlighting the upregulation of the PI3/AKT signalling pathway and increased cAMP levels. These findings shed light on the neuroprotective and anti-inflammatory effects of GLP1-R agonists in HIE, potentially extending to other neurological conditions, supporting their potential clinical use in treating infants with HIE.
Keywords: Exendin-4; GLP1-R Agonists; Neonatal Hypoxic-ischaemic Encephalopathy; Neuroprotective Mechanisms; Semaglutide.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures












References
-
- Athauda D, Maclagan K, Skene SS, Bajwa-Joseph M, Letchford D, Chowdhury K, Hibbert S, Budnik N, Zampedri L, Dickson J, et al. Exenatide once weekly versus placebo in Parkinson’s disease: a randomised, double-blind, placebo-controlled trial. Lancet. 2017;390:1664–1675. doi: 10.1016/S0140-6736(17)31585-4. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
- 204841/Z/16/Z/Wellcome Trust (WT)
- MR/R025134/1/MRC_/Medical Research Council/United Kingdom
- MR/T044853/1/UKRI | Medical Research Council (MRC)
- MR/R025134/1/UKRI | Medical Research Council (MRC)
- MR/S036784/1/MRC_/Medical Research Council/United Kingdom
- MR/N026101/1/UKRI | Medical Research Council (MRC)
- MR/S009434/1/UKRI | Medical Research Council (MRC)
- MR/N026101/1/MRC_/Medical Research Council/United Kingdom
- GN2485/Action Medical Research (AMR)
- MR/T044853/1/MRC_/Medical Research Council/United Kingdom
- 666918/EC | Horizon 2020 Framework Programme (H2020)
- MR/S036784/1/UKRI | Medical Research Council (MRC)
- IS-BRC-1215-20012/NIHR | NIHR Great Ormond Street Hospital Biomedical Research Centre (BRC)
LinkOut - more resources
Full Text Sources
