

Prospective associations of leucocyte subtypes and obesity with the risk of developing cutaneous malignant melanoma in the UK Biobank cohort
- PMID: 38783251
- PMCID: PMC11112846
- DOI: 10.1186/s12885-024-12344-0
Prospective associations of leucocyte subtypes and obesity with the risk of developing cutaneous malignant melanoma in the UK Biobank cohort
Abstract
Background: Obesity is associated with chronic low-grade inflammation, which is linked to cancer development. Abdominal obesity (a body mass index, ABSI), however, has unusually been associated inversely with cutaneous malignant melanoma (CMM), while general obesity (body mass index, BMI) is associated positively. Leucocytes participate in inflammation and are higher in obesity, but prospective associations of leucocytes with cutaneous malignant melanoma are unclear.
Methods: We examined the prospective associations of neutrophil, lymphocyte, and monocyte counts (each individually), as well as the prospective associations of ABSI and BMI, with cutaneous malignant melanoma in UK Biobank. We used multivariable Cox proportional hazards models and explored heterogeneity according to sex, menopausal status, age (≥ 50 years at recruitment), smoking status, ABSI (dichotomised at the median: ≥73.5 women; ≥79.8 men), BMI (normal weight, overweight, obese), and time to diagnosis.
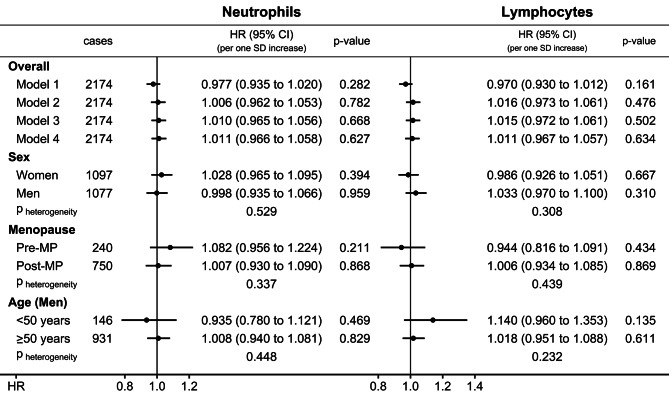
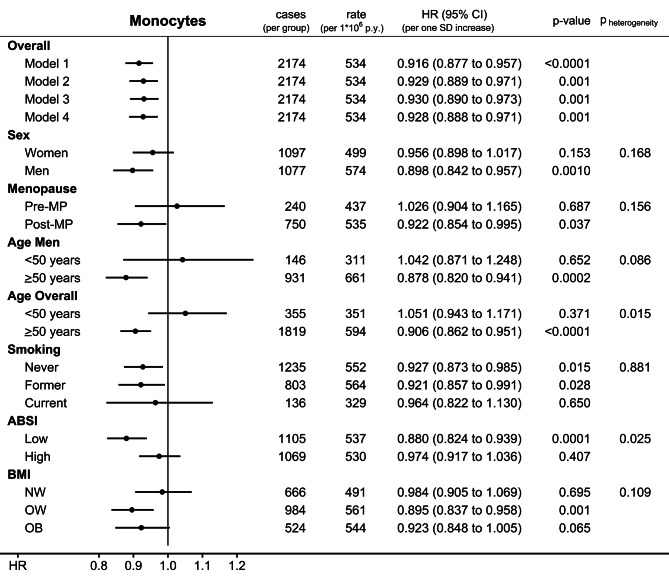
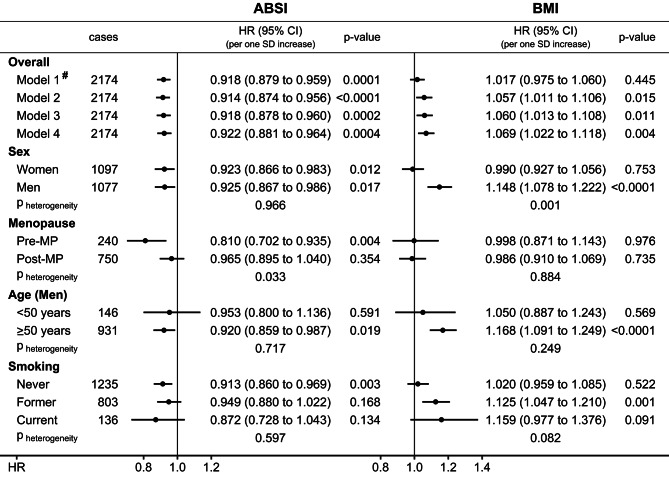
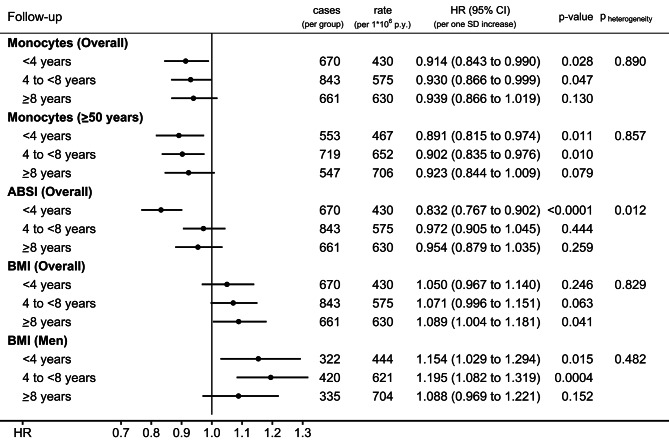
Results: During a mean follow-up of 10.2 years, 2174 CMM cases were ascertained in 398,450 participants. There was little evidence for associations with neutrophil or lymphocyte counts. Monocyte count, however, was associated inversely in participants overall (HR = 0.928; 95%CI: 0.888-0.971; per one standard deviation increase; SD = 0.144*109/L women; SD = 0.169*109/L men), specifically in older participants (HR = 0.906; 95%CI: 0.862-0.951), and more clearly in participants with low ABSI (HR = 0.880; 95%CI: 0.824-0.939), or with BMI ≥ 25 kg/m2 (HR = 0.895; 95%CI: 0.837-0.958 for overweight; HR = 0.923; 95%CI: 0.848-1.005 for obese). ABSI was associated inversely in pre-menopausal women (HR = 0.810; 95%CI: 0.702-0.935; SD = 4.95) and men (HR = 0.925; 95%CI: 0.867-0.986; SD = 4.11). BMI was associated positively in men (HR = 1.148; 95%CI: 1.078-1.222; SD = 4.04 kg/m2). There was little evidence for heterogeneity according to smoking status. The associations with monocyte count and BMI were retained to at least 8 years prior to diagnosis, but the association with ABSI was observed up to 4 years prior to diagnosis and not for longer follow-up time.
Conclusions: Monocyte count is associated prospectively inversely with the risk of developing CMM in older individuals, while BMI is associated positively in men, suggesting a mechanistic involvement of factors related to monocytes and subcutaneous adipose tissue in melanoma development. An inverse association with ABSI closer to diagnosis may reflect reverse causality or glucocorticoid resistance.
Keywords: ABSI; Abdominal obesity; BMI; Cutaneous malignant melanoma; Lymphocytes; Monocytes; Neutrophils; Obesity.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
Associations of obesity and body shape with erythrocyte and reticulocyte parameters in the UK Biobank cohort.BMC Endocr Disord. 2023 Aug 2;23(1):161. doi: 10.1186/s12902-023-01423-1. BMC Endocr Disord. 2023. PMID: 37528422 Free PMC article.
-
A Body Shape Index (ABSI), hip index, and risk of cancer in the UK Biobank cohort.Cancer Med. 2021 Aug;10(16):5614-5628. doi: 10.1002/cam4.4097. Epub 2021 Jul 1. Cancer Med. 2021. PMID: 34196490 Free PMC article.
-
Sex differences in the associations of body size and body shape with platelets in the UK Biobank cohort.Biol Sex Differ. 2023 Feb 22;14(1):12. doi: 10.1186/s13293-023-00494-y. Biol Sex Differ. 2023. PMID: 36814334 Free PMC article.
-
Interactions of platelets with obesity in relation to lung cancer risk in the UK Biobank cohort.Respir Res. 2023 Oct 17;24(1):249. doi: 10.1186/s12931-023-02561-9. Respir Res. 2023. PMID: 37848891 Free PMC article.
-
The Neutrophil-to-Lymphocyte Ratio as a Biomarker in Cutaneous Oncology: A Systematic Review of Evidence beyond Malignant Melanoma.Cancers (Basel). 2024 Mar 4;16(5):1044. doi: 10.3390/cancers16051044. Cancers (Basel). 2024. PMID: 38473401 Free PMC article. Review.
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
