

Prognostic value of early EEG abnormalities in severe stroke patients requiring mechanical ventilation: a pre-planned analysis of the SPICE prospective multicenter study
- PMID: 38783313
- PMCID: PMC11119574
- DOI: 10.1186/s13054-024-04957-5
Prognostic value of early EEG abnormalities in severe stroke patients requiring mechanical ventilation: a pre-planned analysis of the SPICE prospective multicenter study
Abstract
Introduction: Prognostication of outcome in severe stroke patients necessitating invasive mechanical ventilation poses significant challenges. The objective of this study was to assess the prognostic significance and prevalence of early electroencephalogram (EEG) abnormalities in adult stroke patients receiving mechanical ventilation.
Methods: This study is a pre-planned ancillary investigation within the prospective multicenter SPICE cohort study (2017-2019), conducted in 33 intensive care units (ICUs) in the Paris area, France. We included adult stroke patients requiring invasive mechanical ventilation, who underwent at least one intermittent EEG examination during their ICU stay. The primary endpoint was the functional neurological outcome at one year, determined using the modified Rankin scale (mRS), and dichotomized as unfavorable (mRS 4-6, indicating severe disability or death) or favorable (mRS 0-3). Multivariable regression analyses were employed to identify EEG abnormalities associated with functional outcomes.
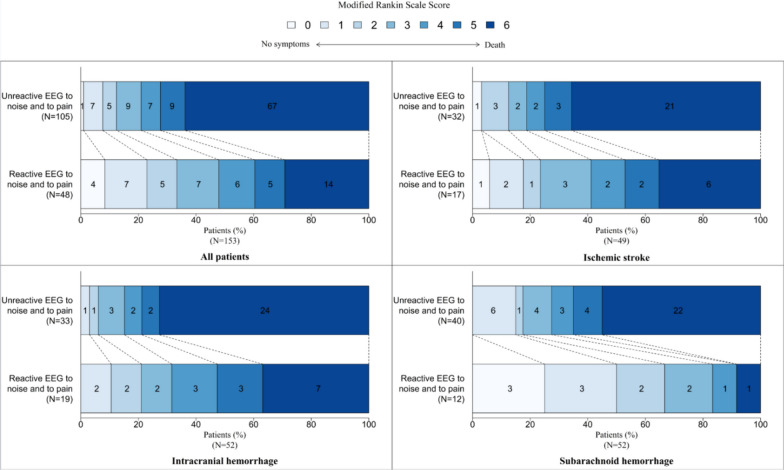
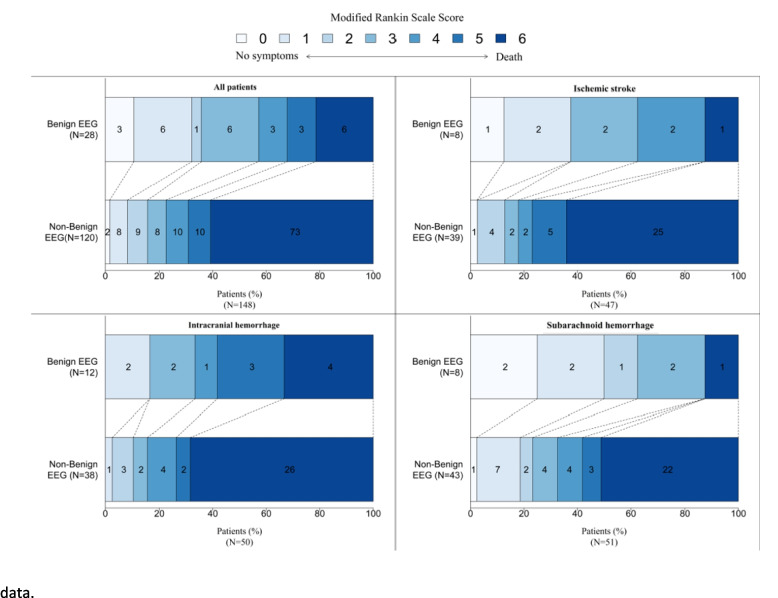
Results: Of the 364 patients enrolled in the SPICE study, 153 patients (49 ischemic strokes, 52 intracranial hemorrhages, and 52 subarachnoid hemorrhages) underwent at least one EEG at a median time of 4 (interquartile range 2-7) days post-stroke. Rates of diffuse slowing (70% vs. 63%, p = 0.37), focal slowing (38% vs. 32%, p = 0.15), periodic discharges (2.3% vs. 3.7%, p = 0.9), and electrographic seizures (4.5% vs. 3.7%, p = 0.4) were comparable between patients with unfavorable and favorable outcomes. Following adjustment for potential confounders, an unreactive EEG background to auditory and pain stimulations (OR 6.02, 95% CI 2.27-15.99) was independently associated with unfavorable outcomes. An unreactive EEG predicted unfavorable outcome with a specificity of 48% (95% CI 40-56), sensitivity of 79% (95% CI 72-85), and positive predictive value (PPV) of 74% (95% CI 67-81). Conversely, a benign EEG (defined as continuous and reactive background activity without seizure, periodic discharges, triphasic waves, or burst suppression) predicted favorable outcome with a specificity of 89% (95% CI 84-94), and a sensitivity of 37% (95% CI 30-45).
Conclusion: The absence of EEG reactivity independently predicts unfavorable outcomes at one year in severe stroke patients requiring mechanical ventilation in the ICU, although its prognostic value remains limited. Conversely, a benign EEG pattern was associated with a favorable outcome.
Keywords: EEG reactivity; Electroencephalogram; Intensive care; Prognostication; Severe stroke.
© 2024. The Author(s).
Conflict of interest statement
None.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
