

N-terminal pro-B-type natriuretic peptide levels pre-transcatheter aortic valve implantation and relationship with long-term outcomes
- PMID: 38784048
- PMCID: PMC11112331
- DOI: 10.1016/j.ijcha.2024.101423
N-terminal pro-B-type natriuretic peptide levels pre-transcatheter aortic valve implantation and relationship with long-term outcomes
Abstract
Background: Blood levels of N-terminal pro-B-type natriuretic peptide (NT-proBNP) has been suggested as a future guidance tool for the selection of patients for aortic valve replacement. This study aimed to examine how levels of NT-proBNP pre-transcatheter aortic valve implantation (TAVI) is associated with one-year rates of heart failure (HF) admission and mortality following TAVI.
Methods: With Danish nationwide registries, we identified all patients undergoing TAVI from 2014 to 2021 who had at least one recorded NT-pro-BNP measurement within one year before TAVI. Patients were compared by quartiles of pre-TAVI NT-proBNP: quartile 4 (high NT-proBNP group) vs quartile 1-3 (low NT-proBNP group). Comparisons of all-cause mortality and HF-admissions were conducted using Kaplan-Meier analysis, cumulative incidence, and Cox analysis, as appropriate.
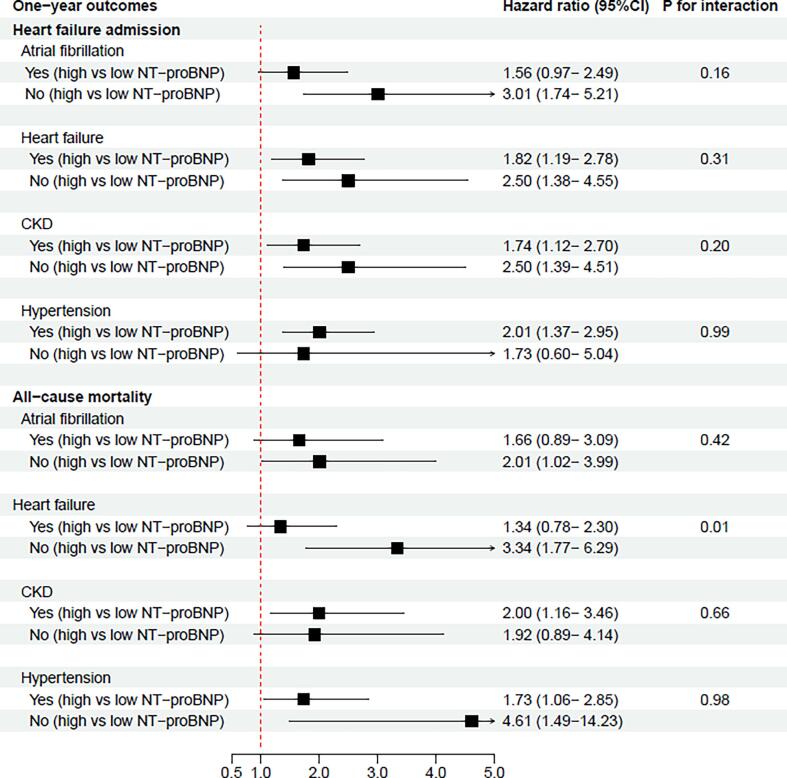
Results: We identified 1,140 patients undergoing first-time TAVI with a recorded NT-pro-BNP; 846 (74.2 %) with a low NT-proBNP (<420 pmol/L) (55.0 % male, median age 81 year) and 294 (25.8 %) with a high NT-proBNP (≥420 pmol/L) (53.1 % male, median age 82 year). A high versus low NT-proBNP was associated with increased one-year cumulative incidence of HF-admissions (9.1 % vs. 23.1 %, adjusted HR 2.00 [95 % CI, 1.40-2.85]) and all-cause mortality (6.0 % vs. 14.6 %, adjusted HR 1.95 [95 % CI: 1.24-3.07]). A high NT-proBNP was associated with higher rates of outcomes irrespective of previously known atrial fibrillation, HF, chronic kidney disease, and hypertension.
Conclusion: In patients undergoing TAVI, a baseline NT-proBNP ≥ 420 pmol/L was associated with increased one-year rates of HF-admission and mortality post-TAVI and may be utilized to identify a high-risk population.
Keywords: Aortic Stenosis; Aortic Valve Replacement; Implantation; N-Terminal Pro-B-Type Natriuretic Peptide; NT-proBNP; TAVI; Transcatheter Aortic Valve.
© 2024 The Author(s).
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures



References
-
- Carroll J.D., et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76(21):2492–2516. - PubMed
-
- Paradies V., Mamas M.A. Aortic valve treatment: from the first aortic valve replacement to the last decade of revolution. Heart. 2023;109(7):502–503. - PubMed
-
- Siontis G.C.M., et al. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. 2019;40(38):3143–3153. - PubMed
-
- Qi W., et al. Natriuretic peptides in patients with aortic stenosis. Am Heart J. 2001;142(4):725–732. - PubMed
-
- Logeart D., et al. Predischarge B-type natriuretic peptide assay for identifying patients at high risk of re-admission after decompensated heart failure. J Am Coll Cardiol. 2004;43(4):635–641. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
