

Persistence and risk factors of occult hepatitis B virus infections among antiretroviral therapy-naïve people living with HIV in Botswana
- PMID: 38784816
- PMCID: PMC11112038
- DOI: 10.3389/fmicb.2024.1342862
Persistence and risk factors of occult hepatitis B virus infections among antiretroviral therapy-naïve people living with HIV in Botswana
Abstract
Aim: This study aimed to determine the kinetics of occult hepatitis B virus infections (OBI) among people with HIV (PWH).
Methods: The study used archived plasma samples from longitudinal HIV natural history studies. We identified new OBI cases and assessed risk factors for OBI using Cox proportional hazards regression analysis.
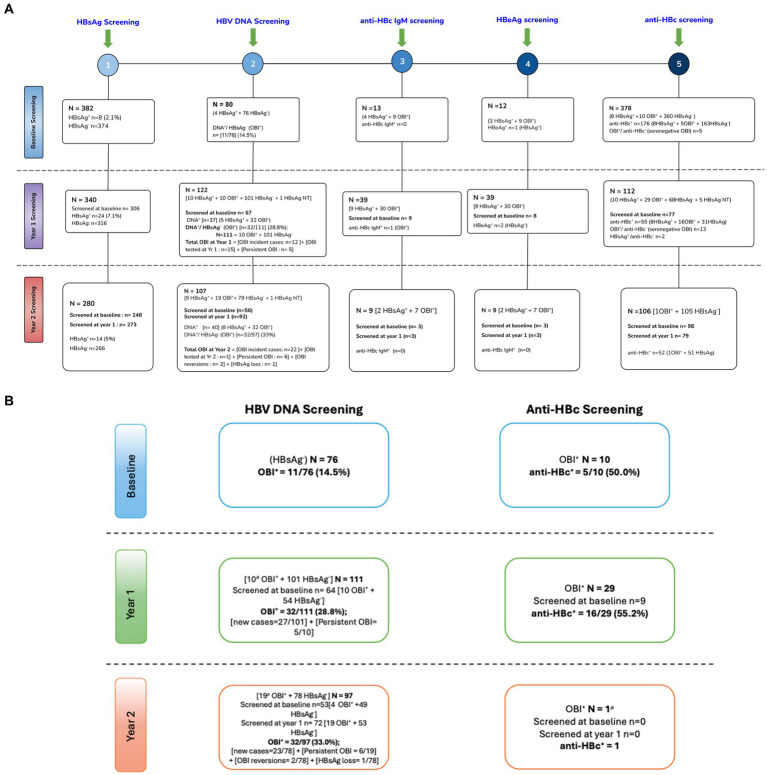
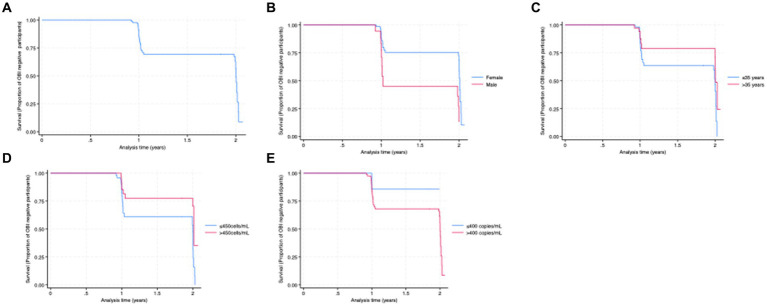
Results: At baseline, 8 of 382 [(2.1%) (95% CI: 1.06-4.1)] samples tested positive for hepatitis B surface antigen (HBsAg+). Of the 374 HBsAg-negative samples, 76 had sufficient sample volume for HBV DNA screening. OBI positivity (OBI+) at baseline was reported in 11 of 76 [14.7 95% CI (8.3-24.1)] HBsAg-negative (HBsAg-) participants. Baseline HBsAg-negative samples with sufficient follow-up samples (n = 90) were used for analysis of newly identified OBI cases. Participants contributed 129.74 person-years to the study and were followed for a median of 1.02 years (IQR: 1.00-2.00). Cumulatively, there were 34 newly identified OBI cases from the 90 participants, at the rate of 26.2/100 person-years (95% CI: 18.7-36.7). Newly identified OBI cases were more common among men than women (61.1% vs. 31.9%) and among participants with CD4+ T-cell counts ≤450 cells/mL (p-value = 0.02). Most of the newly identified OBI cases [55.9% (19/34)] were possible reactivations as they were previously HBV core antibody positive.
Conclusion: There was a high rate of newly identified OBI among young PWH in Botswana, especially in men and in participants with lower CD4+ T-cell counts. OBI screening in PWH should be considered because of the risk of transmission, possible reactivation, and risk factors for the development of chronic liver disease, including hepatocellular carcinoma.
Keywords: HBV; HIV/HBV, hepatitis B surface antigen (HBsAg) negative; OBI; hepatitis B virus; incidence; occult hepatitis B.
Copyright © 2024 Anderson, Phinius, Phakedi, Mudanga, Bhebhe, Tlhabano, Motshosi, Ratsoma, Baruti, Mpebe, Choga, Marlink, Glebe, Blackard, Moyo, Kramvis and Gaseitsiwe.
Conflict of interest statement
AK is the Specialty Chief Editor of the Virology Section of Frontiers in Microbiology. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. The reviewer WG declared a shared affiliation with the author DG to the handling editor at the time of review. The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Figures
Similar articles
-
Prevalence of occult hepatitis B infection among treatment-naive persons living with HIV in Ghana.PLoS One. 2024 Jun 26;19(6):e0305862. doi: 10.1371/journal.pone.0305862. eCollection 2024. PLoS One. 2024. PMID: 38924017 Free PMC article.
-
Occult hepatitis B virus infection in a Kenyan cohort of HIV infected anti-retroviral therapy naïve adults.PLoS One. 2021 Jan 6;16(1):e0244947. doi: 10.1371/journal.pone.0244947. eCollection 2021. PLoS One. 2021. PMID: 33406137 Free PMC article.
-
[Prevalence of viral hepatitis B markers among blood donors in the Republic of Guinea].Vopr Virusol. 2022 Mar 15;67(1):59-68. doi: 10.36233/0507-4088-92. Vopr Virusol. 2022. PMID: 35293189 Russian.
-
Management of occult hepatitis B virus infection: an update for the clinician.World J Gastroenterol. 2011 Mar 28;17(12):1563-8. doi: 10.3748/wjg.v17.i12.1563. World J Gastroenterol. 2011. PMID: 21472122 Free PMC article. Review.
-
Occult hepatitis B virus infection: detection and significance.Dig Dis. 2010;28(1):116-25. doi: 10.1159/000282074. Epub 2010 May 7. Dig Dis. 2010. PMID: 20460899 Review.
Cited by
-
The miRNomics of antiretroviral therapy-induced obesity.Funct Integr Genomics. 2025 Apr 5;25(1):81. doi: 10.1007/s10142-025-01585-2. Funct Integr Genomics. 2025. PMID: 40186666 Free PMC article. Review.
References
-
- Amponsah-Dacosta E., Lebelo R. L., Rakgole J. N., Selabe S. G., Gededzha M. P., Mayaphi S. H., et al. . (2015). Hepatitis B virus infection in post-vaccination South Africa: occult HBV infection and circulating surface gene variants. J. Clin. Virol. 63, 12–17. doi: 10.1016/j.jcv.2014.11.032, PMID: - DOI - PMC - PubMed
-
- Anderson M., Choga W. T., Moyo S., Bell T. G., Mbangiwa T., Phinius B. B., et al. . (2018a). Molecular characterization of near full-length genomes of hepatitis B virus isolated from predominantly HIV infected individuals in Botswana. Genes (Basel) 9, 1–20. doi: 10.3390/genes9090453, PMID: - DOI - PMC - PubMed
-
- Anderson M., Gaseitsiwe S., Moyo S., Thami K. P., Mohammed T., Setlhare D., et al. . (2016). Slow CD4+ T-cell recovery in human immunodeficiency virus/hepatitis B virus-Coinfected patients initiating Truvada-based combination antiretroviral therapy in Botswana. Infect. Dis. 3, 1–8. doi: 10.1093/ofid/ofw140 - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials