

Infected Post-traumatic Bone Defect of the Knee using Bipolar Osteochondral Allograft and 3D Printing: A Case Report
- PMID: 38784883
- PMCID: PMC11111241
- DOI: 10.13107/jocr.2024.v14.i05.4452
Infected Post-traumatic Bone Defect of the Knee using Bipolar Osteochondral Allograft and 3D Printing: A Case Report
Abstract
Introduction: Transplantation with fresh cadaveric osteochondral allograft (FOCA) is frequently used in defects of the femoral condyle and tibial plateau to preserve the knee joint. However, the use of FOCA in bipolar lesions remains controversial in cases with bipolar defects and a history of infection.
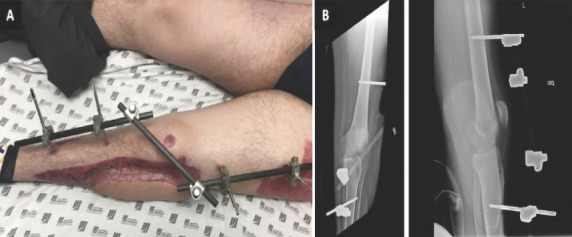
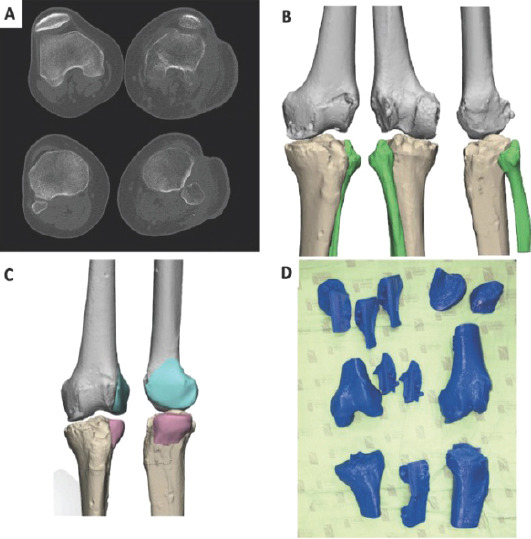
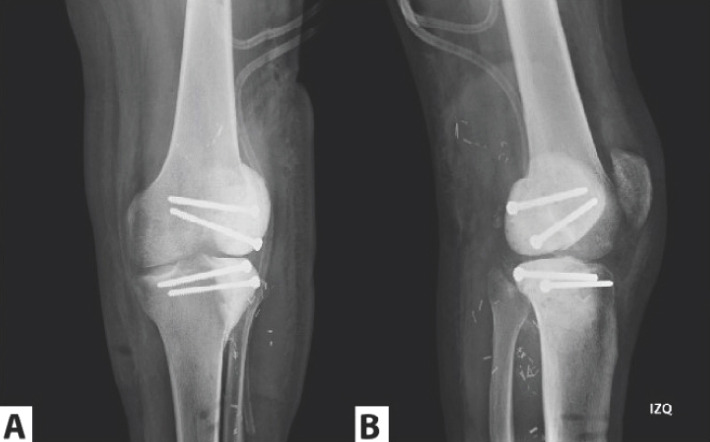
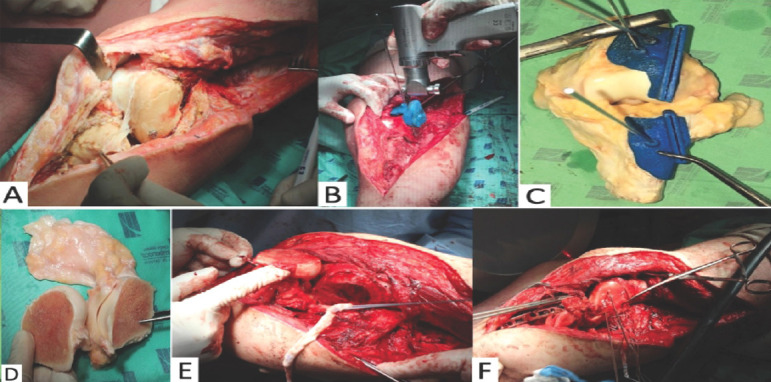
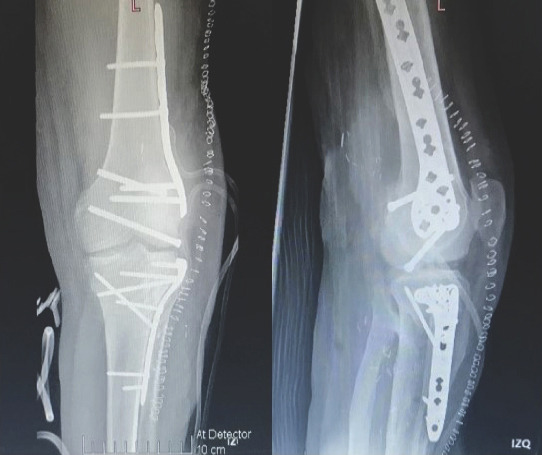
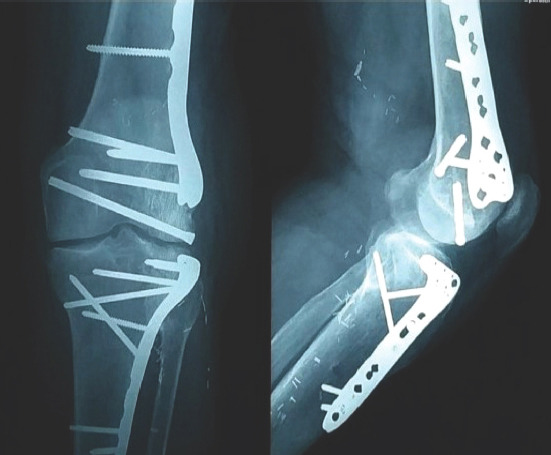
Case report: We present a 21-year-old male patient with a massive post-traumatic osteochondral defect of the lateral compartment of the knee and a history of infection, treated by a two-stage approach. In stage 1, infection was eradicated, and joint function recovered with aggressive debridement, polymethyl methacrylate beads, bone cement spacers, and Judet's quadricepsplasty. In stage 2, transplantation was performed with a bipolar FOCA. All treatments were planned using 3D-printed models.
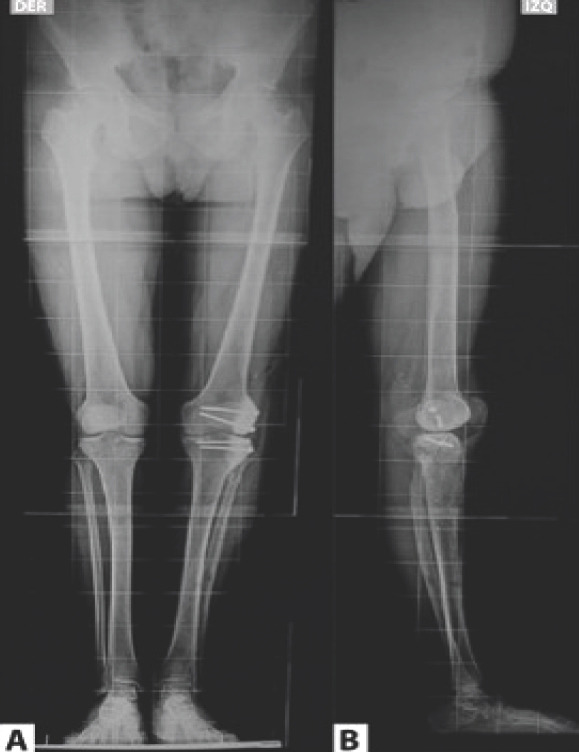
Conclusion: The two-stage approach and 3D planning can increase the chances of transplant success by preparing the future allograft bed and obtaining an optimal match between the cadaveric allograft and the patient's defect in cases with potential contraindications, such as a bipolar lesion in the femoral condyle and tibial plateau and a history of infection. A combined approach may lead to a more beneficial outcome for the patient to preserve joint function and improve quality of life.
Keywords: 3D planning; Osteochondral allograft; bone defect.
Copyright: © Indian Orthopaedic Research Group.
Conflict of interest statement
Conflict of Interest: None
Figures
Similar articles
-
Osteochondral Allograft Transplantation for Focal Cartilage Defects of the Femoral Condyles.JBJS Essent Surg Tech. 2022 Sep 22;12(3):e21.00037. doi: 10.2106/JBJS.ST.21.00037. eCollection 2022 Jul-Sep. JBJS Essent Surg Tech. 2022. PMID: 36816528 Free PMC article.
-
Osteochondral Allograft Transplantation for a Large Focal Osteochondral Defect of the Lateral Femoral Condyle: Technical Note and Case Report.J Orthop Case Rep. 2025 Apr;15(4):199-204. doi: 10.13107/jocr.2025.v15.i04.5498. J Orthop Case Rep. 2025. PMID: 40212491 Free PMC article.
-
Distal femoral varus osteotomy combined with tibial plateau fresh osteochondral allograft for post-traumatic osteoarthritis of the knee.Knee Surg Sports Traumatol Arthrosc. 2015 May;23(5):1317-1323. doi: 10.1007/s00167-013-2828-x. Epub 2014 Jan 14. Knee Surg Sports Traumatol Arthrosc. 2015. PMID: 24420606
-
Isolated Osteochondral Autograft Versus Allograft Transplantation for the Treatment of Symptomatic Cartilage Lesions of the Knee: A Systematic Review and Meta-analysis.Am J Sports Med. 2023 Mar;51(3):812-824. doi: 10.1177/03635465211053594. Epub 2022 Feb 9. Am J Sports Med. 2023. PMID: 35139311
-
Fresh Osteochondral Allograft Transplantation in Osteochondritis Dissecans in the Knee Joint.Life (Basel). 2021 Nov 8;11(11):1205. doi: 10.3390/life11111205. Life (Basel). 2021. PMID: 34833081 Free PMC article. Review.
References
-
- Cavendish PA, Everhart JS, Peters NJ, Sommerfeldt MF, Flanigan DC. Osteochondral allograft transplantation for knee cartilage and osteochondral defects:A review of indications, technique, rehabilitation, and outcomes. JBJS Rev. 2019;7:e7. - PubMed
-
- Hohmann E, Tetsworth K. Large osteochondral lesions of the femoral condyles:Treatment with fresh frozen and irradiated allograft using the Mega OATS technique. Knee. 2016;23:436–41. - PubMed
-
- Schmidt KJ, Tírico LE, McCauley JC, Bugbee WD. Fresh osteochondral allograft transplantation:Is graft storage time associated with clinical outcomes and graft survivorship? Am J Sports Med. 2017;45:2260–6. - PubMed
Publication types
LinkOut - more resources
Full Text Sources