

Cholesteryl Ester Transfer Protein Inhibitors and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis
- PMID: 38786974
- PMCID: PMC11122262
- DOI: 10.3390/jcdd11050152
Cholesteryl Ester Transfer Protein Inhibitors and Cardiovascular Outcomes: A Systematic Review and Meta-Analysis
Abstract
Background: Atherosclerosis is a multi-factorial disease, and low-density lipoprotein cholesterol (LDL-C) is a critical risk factor in developing atherosclerotic cardiovascular disease (ASCVD). Cholesteryl-ester transfer-protein (CETP), synthesized by the liver, regulates LDL-C and high-density lipoprotein cholesterol (HDL-C) through the bidirectional transfer of lipids. The novelty of CETP inhibitors (CETPis) has granted new focus towards increasing HDL-C, besides lowering LDL-C strategies. To date, five CETPis that are projected to improve lipid profiles, torcetrapib, dalcetrapib, evacetrapib, anacetrapib, and obicetrapib, have reached late-stage clinical development for ASCVD risk reduction. Early trials failed to reduce atherosclerotic cardiovascular occurrences. Given the advent of some recent large-scale clinical trials (ACCELERATE, HPS3/TIMI55-REVEAL Collaborative Group), conducting a meta-analysis is essential to investigate CETPis' efficacy.
Methods: We conducted a thorough search of randomized controlled trials (RCTs) that commenced between 2003 and 2023; CETPi versus placebo studies with a ≥6-month follow-up and defined outcomes were eligible.
Primary outcomes: major adverse cardiovascular events (MACEs), cardiovascular disease (CVD)-related mortality, all-cause mortality.
Secondary outcomes: stroke, revascularization, hospitalization due to acute coronary syndrome, myocardial infarction (MI).
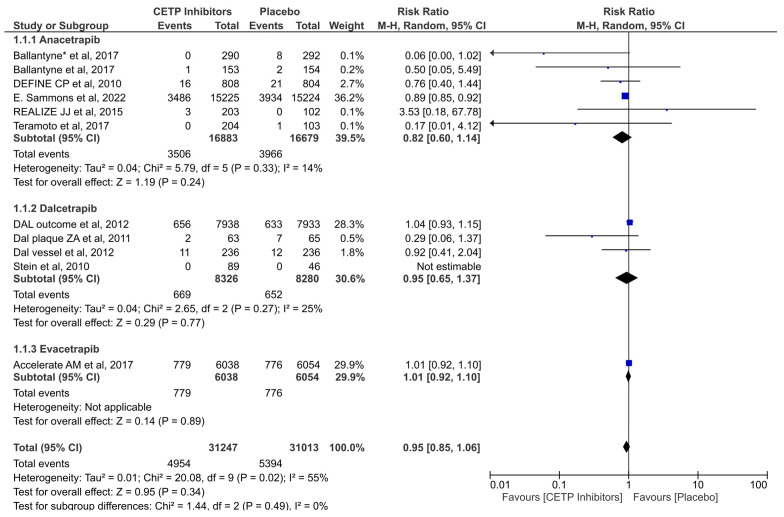
Results: Nine RCTs revealed that the use of a CETPi significantly reduced CVD-related mortality (RR = 0.89; 95% CI: 0.81-0.98; p = 0.02; I2 = 0%); the same studies also reduced the risk of MI (RR = 0.92; 95% CI: 0.86-0.98; p = 0.01; I2 = 0%), which was primarily attributed to anacetrapib. The use of a CETPi did not reduce the likelihood any other outcomes.
Conclusions: Our meta-analysis shows, for the first time, that CETPis are associated with reduced CVD-related mortality and MI.
Keywords: CETP inhibitors; HDL-C lipoproteins; LDL-C lipoproteins; anacetrapib; atherosclerosis; cholesterol ester transfer protein; dalceprapib; evacetrapib; obicetrapib; torcetrapib.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures




References
-
- Cholesterol Treatment Trialists’ (CTT) Collaboration. Baigent C., Blackwell L., Emberson J., Holland L.E., Reith C., Bhala N., Peto R., Barnes E.H., Keech A., et al. Efficacy and safety of more intensive lowering of LDL cholesterol: A meta-analysis of data from 170,000 participants in 26 randomised trials. Lancet. 2010;376:1670–1681. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
