

Evaluating use of two-step International Ovarian Tumor Analysis strategy to classify adnexal masses identified in pregnancy: pilot study
- PMID: 38787921
- PMCID: PMC11609963
- DOI: 10.1002/uog.27707
Evaluating use of two-step International Ovarian Tumor Analysis strategy to classify adnexal masses identified in pregnancy: pilot study
Abstract
Objectives: The primary aim was to validate the International Ovarian Tumor Analysis (IOTA) benign simple descriptors (BDs) followed by the Assessment of Different NEoplasias in the adneXa (ADNEX) model, if BDs cannot be applied, in a two-step strategy to classify adnexal masses identified during pregnancy. The secondary aim was to describe the natural history of adnexal masses during pregnancy.
Methods: This was a retrospective analysis of prospectively collected data from women with an adnexal mass identified on ultrasonography during pregnancy between 2017 and 2022 at Queen Charlotte's and Chelsea Hospital, London, UK. Clinical and ultrasound data were extracted from medical records and ultrasound software. Adnexal masses were classified and managed according to expert subjective assessment (SA). Borderline ovarian tumors (BOTs) were classified as malignant. BDs were applied retrospectively to classify adnexal masses, and if BDs were not applicable, the ADNEX model (using a risk- of-malignancy threshold ≥ 10%) was used, in a two-step strategy. The reference standard was histology (where available) or expert SA at the postnatal ultrasound scan.
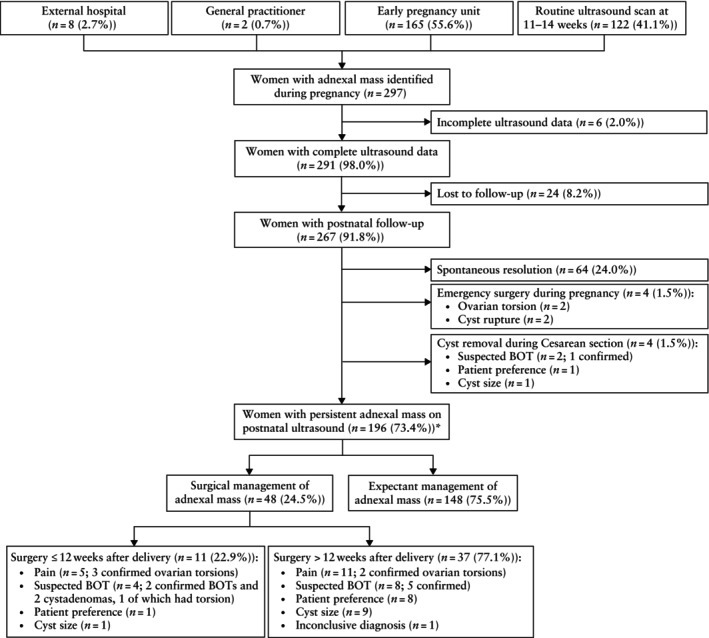
Results: A total of 291 women with a median age of 33 (interquartile range (IQR), 29-36) years presented with an adnexal mass during pregnancy, at a median gestational age of 12 (IQR, 8-17) weeks. Of those, 267 (91.8%) were followed up to the postnatal period. Based on the reference standard, 4.1% (11/267) of adnexal masses were classified as malignant (all BOTs) and 95.9% (256/267) as benign. BDs were applicable in 68.9% (184/267) of adnexal masses; of these, only one (0.5%) BOT was misclassified as benign. The ADNEX model was used to classify the 83 residual masses and misclassified 3/10 (30.0%) BOTs as benign and 25/73 (34.2%) benign masses as malignant, of which 13/25 (52.0%) were classified as decidualized endometrioma on expert SA. The two-step strategy had a specificity of 90.2%, sensitivity of 63.6%, negative predictive value of 98.3% and positive predictive value of 21.9%. A total of 56 (21.0%) women underwent surgical intervention: four (1.5%) as an emergency during pregnancy, four (1.5%) electively during Cesarean section and 48 (18.0%) postnatally. During follow-up, 64 (24.0%) adnexal masses resolved spontaneously. Cyst-related complications occurred in four (1.5%) women during pregnancy (ovarian torsion, n = 2; cyst rupture, n = 2) and six (2.2%) women in the postnatal period (all ovarian torsion). Overall, 196/267 (73.4%) women had a persistent adnexal mass at postnatal ultrasound. Presumed decidualization occurred in 31.1% (19/61) of endometriomas and had resolved in 89.5% (17/19) by the first postnatal ultrasound scan.
Conclusions: BDs apply to most adnexal masses during pregnancy. However, the small number of malignant tumors in this cohort (4.1%) restricted the evaluation of the ADNEX model, so expert SA should be used to classify adnexal masses during pregnancy when BDs do not apply. A larger multicenter prospective study is required to evaluate the use of the ADNEX model to classify adnexal masses during pregnancy. Our data suggest that most adnexal masses can be managed expectantly during pregnancy, given the high rate of spontaneous resolution and low risk of complications. © 2024 The Author(s). Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
RESUMEN: Evaluación del uso de la estrategia internacional de análisis de tumores ováricos en dos pasos para clasificar masas anexiales identificadas en el embarazo: un estudio piloto.
Objetivos: El objetivo principal fue validar los descriptores benignos (DB) simples del Análisis Internacional de Tumores Ováricos (IOTA, por sus siglas en inglés) seguidos de la Evaluación de Diferentes Neoplasias en el modelo adneXa (ADNEX), si no se pueden aplicar los DB, en una estrategia de dos pasos para clasificar las masas anexiales identificadas durante el embarazo. El objetivo secundario fue describir el historial natural de las masas anexiales durante el embarazo.
Métodos: Se realizó un análisis retrospectivo de datos recopilados prospectivamente de mujeres con una masa anexial identificada en la ecografía durante el embarazo entre 2017 y 2022 en el hospital Queen Charlotte's and Chelsea de Londres (Reino Unido). Los datos clínicos y ecográficos se obtuvieron de los historiales clínicos y del programa informático de ecografía. Las masas anexiales se clasificaron y trataron según la evaluación subjetiva (ES) por expertos. Los tumores ováricos limítrofes (TOL) se clasificaron como malignos. Los DB se aplicaron retrospectivamente para clasificar las masas anexiales, y si los DB no eran aplicables, se utilizó el modelo ADNEX (utilizando un umbral de riesgo de malignidad ≥10%), en una estrategia de dos pasos. El estándar de referencia fue la histología (cuando estaba disponible) o la ES por expertos en ecografía postnatal.
Resultados: Un total de 291 mujeres con una mediana de edad de 33 años (rango intercuartílico [RIQ], 29–36) presentaron una masa anexial durante el embarazo, a una mediana de edad gestacional de 12 semanas (RIQ, 8–17). De ellas, a 267 (91,8%) se les dio seguimiento hasta el periodo postnatal. Según el estándar de referencia, el 4,1% (11/267) de las masas anexiales se clasificaron como malignas (todas TOL) y el 95,9% (256/267) como benignas. Los DB fueron aplicables al 68,9% (184/267) de las masas anexiales; de éstas, sólo un TOL (0,5%) se clasificó erróneamente como benigno. Se utilizó el modelo ADNEX para clasificar las 83 masas residuales y se clasificaron 3/10 (30,0%) TOL como benignas y 25/73 (34,2%) masas benignas como malignas, de las cuales 13/25 (52,0%) se clasificaron como endometrioma decidualizado en la ES por expertos. La estrategia en dos pasos tuvo una especificidad del 90,2%, una sensibilidad del 63,6%, un valor predictivo negativo del 98,3% y un valor predictivo positivo del 21,9%. Un total de 56 (21,0%) mujeres se sometieron a una intervención quirúrgica: cuatro (1,5%) como urgencia durante el embarazo, cuatro (1,5%) de forma electiva durante una cesárea y 48 (18,0%) en el posparto. Durante el seguimiento, 64 (24,0%) masas anexiales se resolvieron espontáneamente. Se produjeron complicaciones relacionadas con quistes en cuatro (1,5%) mujeres durante el embarazo (torsión ovárica, n=2; rotura de quiste, n=2) y en seis (2,2%) mujeres en el periodo postnatal (todas torsión ovárica). En total, 196/267 (73,4%) mujeres presentaban una masa anexial persistente en la ecografía postnatal. La presunta decidualización se produjo en el 31,1% (19/61) de los endometriomas y el 89,5% (17/19) se habían resuelto en la primera ecografía postnatal.
Conclusiones: Los DB aplican a la mayoría de las masas anexiales durante el embarazo. Sin embargo, el escaso número de tumores malignos en esta cohorte (4,1%) restringió la evaluación del modelo ADNEX, por lo que cuando no apliquen los DB debería recurrirse a la ES por expertos para clasificar las masas anexiales durante el embarazo. Se requiere un estudio prospectivo multicéntrico más amplio para evaluar el uso del modelo ADNEX para clasificar las masas anexiales durante el embarazo. Los datos de este estudio sugieren que la mayoría de las masas anexiales pueden tratarse de forma expectante durante el embarazo, dada la alta tasa de resolución espontánea y el bajo riesgo de complicaciones.
摘要: 评估使用国际卵巢肿瘤研究组两步策略对妊娠期发现的附件肿块进行分类:试点研究
目的: 主要目的是先验证国际卵巢肿瘤研究组(IOTA)的良性简单描述符(BD),如果无法应用BD,则使用多元附件肿瘤评估模型ADNEX,
分两步对妊娠期间发现的附件肿块进行分类。第二目的是描述妊娠期间附件肿块的自然病史。
方法: 本研究为对英国伦敦夏洛特女王和切尔西医院(Queen Charlotte's and Chelsea Hospital) 2017 年至 2022 年期间前瞻性收集的孕期超声检查发现附件肿块的妇女数据进行的回顾性分析。临床和超声数据均从医疗记录和超声软件中提取。附件肿块根据专家主观评估(SA)进行分类和管理。卵巢交界性肿瘤(BOT)被归类为恶性肿瘤。回顾性应用 BD 对附件肿块进行分类,如果 BD 不适用,则采用 ADNEX 模型(恶性风险阈值≥10%),分两步进行。参考标准为组织学检查(如有)或产后超声扫描的专家SA。
结果: 共有 291 名中位数年龄为 33 岁(四分位距(IQR)为 29‐36 岁)的妇女在妊娠期间出现附件肿块,中位数孕周为 12 周(IQR 为 8‐17 周)。其中 267 人(91.8%)接受了产后随访。根据参考标准,4.1%(11/267)的附件肿块被归类为恶性(均为 BOT),95.9%(256/267)被归类为良性。68.9%(184/267)的附件肿块适用 Bd;其中只有 1 例(0.5%)BOT 被误判为良性。使用 ADNEX 模型对剩余 83 例肿块进行分类,其中 3/10(30.0%)例 BOT 被归类为良性,25/73(34.2%)例良性肿块被归类为恶性,其中 13/25(52.0%)例根据专家 SA 被归类为蜕膜化子宫内膜异位。两步法的特异性为 90.2%,敏感性为 63.6%,阴性预测值为 98.3%,阳性预测值为 21.9%。共有 56 名(21.0%)妇女接受了手术治疗:其中 4 名(1.5%)是孕期急诊,4 名(1.5%)是剖宫产期间选择性治疗,48 名(18.0%)是产后治疗。在随访期间,64 例(24.0%)附件肿块自行消退。有 4 名(1.5%)妇女在孕期发生了与囊肿相关的并发症(卵巢扭转,2 例;囊肿破裂,2 例),有 6 名(2.2%)妇女在产后发生了与囊肿相关的并发症(均为卵巢扭转)。总体而言,196/267(73.4%)名妇女在产后超声检查中发现有持续性附件肿块。31.1%(19/61)的子宫内膜异位症推断发生了蜕膜化,89.5%(17/19)的子宫内膜异位症在产后第一次超声检查时已经消退。
结论: BD 适用于孕期的大多数附件肿块。然而,由于本队列中恶性肿瘤的数量较少(4.1%),限制了对 ADNEX 模型的评估,因此当 BD 不适用时,应使用专家 SA 对孕期附件肿块进行分类。需要进行更大规模的多中心前瞻性研究,以评估使用 ADNEX 模型对孕期附件肿块进行分类的效果。我们的数据表明,鉴于附件肿块的自行消退率高且并发症风险低,大多数妊娠期附件肿块可作期待治疗。
Keywords: ADNEX model; benign simple descriptor; classification; ovarian cancer; ovarian cyst; pregnancy; ultrasonography; validation.
© 2024 The Author(s). Ultrasound in Obstetrics & Gynecology published by John Wiley & Sons Ltd on behalf of International Society of Ultrasound in Obstetrics and Gynecology.
Figures
Similar articles
-
Prospective external validation of IOTA methods for classifying adnexal masses and retrospective assessment of two-step strategy using benign descriptors and ADNEX model: Portuguese multicenter study.Ultrasound Obstet Gynecol. 2024 Oct;64(4):538-549. doi: 10.1002/uog.27641. Epub 2024 Sep 4. Ultrasound Obstet Gynecol. 2024. PMID: 38477149
-
Validation of ADNEX and IOTA two-step strategy and estimation of risk of complications during follow-up of adnexal masses in low-risk population.Ultrasound Obstet Gynecol. 2024 Sep;64(3):395-404. doi: 10.1002/uog.27642. Epub 2024 Aug 16. Ultrasound Obstet Gynecol. 2024. PMID: 38477179
-
Benign descriptors and ADNEX in two-step strategy to estimate risk of malignancy in ovarian tumors: retrospective validation in IOTA5 multicenter cohort.Ultrasound Obstet Gynecol. 2023 Feb;61(2):231-242. doi: 10.1002/uog.26080. Epub 2023 Jan 12. Ultrasound Obstet Gynecol. 2023. PMID: 36178788 Free PMC article.
-
Adnexal masses during pregnancy: diagnosis, treatment, and prognosis.Am J Obstet Gynecol. 2023 Jun;228(6):601-612. doi: 10.1016/j.ajog.2022.11.1291. Epub 2022 Nov 19. Am J Obstet Gynecol. 2023. PMID: 36410423 Review.
-
Management of the adnexal mass in pregnancy.Curr Opin Obstet Gynecol. 2014 Apr;26(2):49-53. doi: 10.1097/GCO.0000000000000048. Curr Opin Obstet Gynecol. 2014. PMID: 24614018 Review.
References
-
- Condous G, Khalid A, Okaro E, Bourne T. Should we be examining the ovaries in pregnancy? Prevalence and natural history of adnexal pathology detected at first‐trimester sonography. Ultrasound Obstet Gynecol. 2004;24(1):62‐66. - PubMed
-
- Yazbek J, Salim R, Woelfer B, Aslam N, Lee CT, Jurkovic D. The value of ultrasound visualization of the ovaries during the routine 11‐14 weeks nuchal translucency scan. Eur J Obstet Gynecol Reprod Biol. 2007;132(2):154‐158. - PubMed
-
- Froyman W, Landolfo C, De Cock B, et al. Risk of complications in patients with conservatively managed ovarian tumours (IOTA5): a 2‐year interim analysis of a multicentre, prospective, cohort study. Lancet Oncol. 2019;20(3):448‐458. - PubMed
-
- Testa AC, Mascilini F, Quagliozzi L, et al. Management of ovarian masses in pregnancy: patient selection for interventional treatment. Int J Gynecol Cancer. 2021;31(6):899‐906. - PubMed
-
- Balinskaite V, Bottle A, Sodhi V, et al. The risk of adverse pregnancy outcomes following nonobstetric surgery during pregnancy: estimates from a retrospective cohort study of 6.5 million pregnancies. Ann Surg. 2017;266(2):260‐266. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
