

Dolutegravir plus boosted darunavir versus recommended standard-of-care antiretroviral regimens in people with HIV-1 for whom recommended first-line non-nucleoside reverse transcriptase inhibitor therapy has failed (D2EFT): an open-label, randomised, phase 3b/4 trial
- PMID: 38788744
- PMCID: PMC11700562
- DOI: 10.1016/S2352-3018(24)00089-4
Dolutegravir plus boosted darunavir versus recommended standard-of-care antiretroviral regimens in people with HIV-1 for whom recommended first-line non-nucleoside reverse transcriptase inhibitor therapy has failed (D2EFT): an open-label, randomised, phase 3b/4 trial
Abstract
Background: Randomised comparative data on efficacy and safety of second-line antiretroviral therapy (ART) after failure of non-nucleoside reverse transcriptase inhibitors (NNRTIs) across diverse geographical settings are scarce. The aim of this study was to evaluate optimal second-line ART for people with HIV.
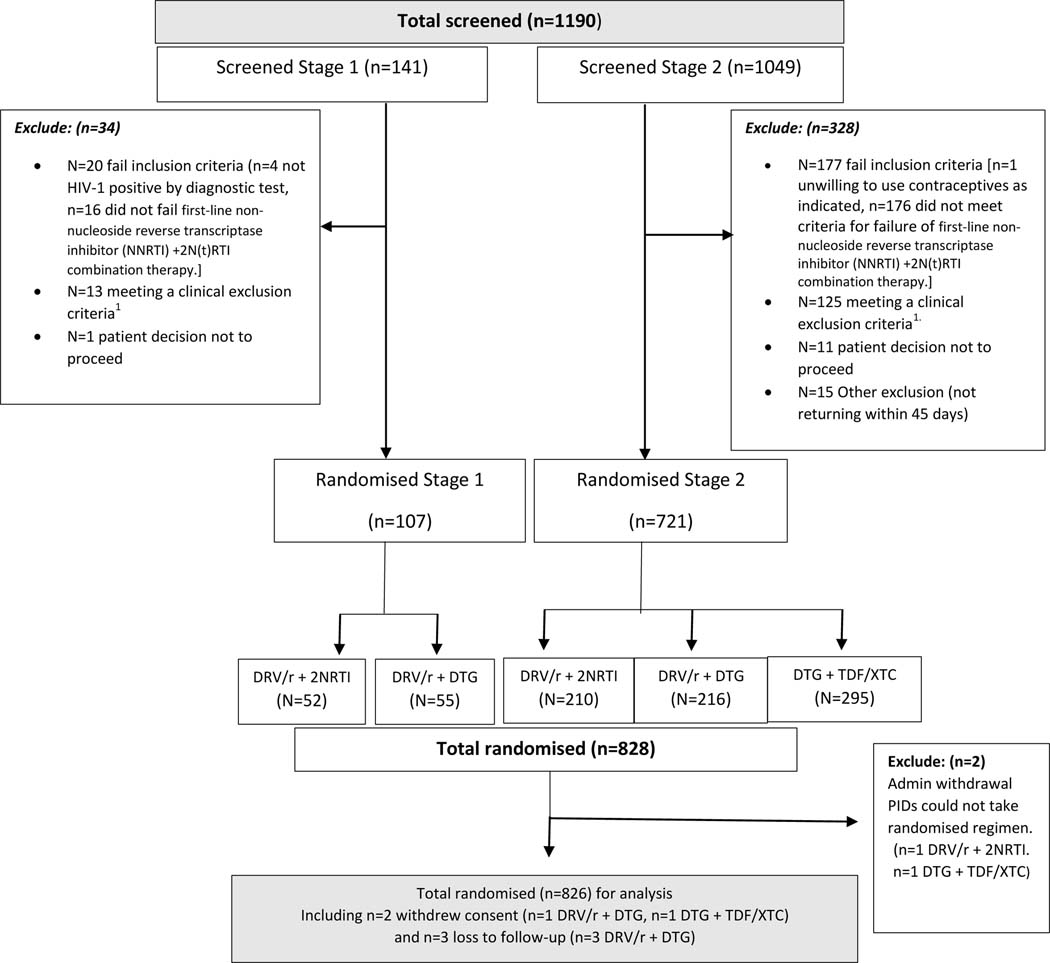
Methods: D2EFT is a completed international, randomised, open-label, phase 3b/4 trial evaluating three second-line ART strategies in adults (aged ≥18 years) with HIV-1 for whom first-line NNRTI therapy has failed. The study was done at 28 sites across 14 countries in Asia, Africa, and Latin America. It was originally designed to compare recommended standard of care (ritonavir-boosted darunavir [800 mg darunavir plus 100 mg ritonavir once daily] plus two nucleoside reverse transcriptase inhibitors [NRTIs; dosed once or twice daily]) with a novel nucleoside sparing regimen of dolutegravir (50 mg once daily) with ritonavir-boosted darunavir. The study was adapted during the first year to add a third arm of dolutegravir (50 mg once daily) with fixed tenofovir disoproxil fumarate (300 mg once daily) plus either lamivudine (300 mg once daily) or emtricitabine (200 mg once daily). Participants were randomly assigned with a computer-generated, blocked randomisation scheme (block size of two) stratified by site, previous tenofovir disoproxil fumarate use, and HIV viral load. The trial was designed to evaluate non-inferiority of either interventional arm against standard of care for the primary outcome of virological suppression, as determined by HIV RNA load of less than 50 copies per mL at 48 weeks. The prespecified non-inferiority margin was 12%. Comparisons were made with a modified intention-to-treat population, including all participants randomly assigned but excluding administrative withdrawals. This study is registered with ClinicalTrials.gov, NCT03017872.
Findings: 1190 individuals were screened; 828 participants were enrolled between Nov 1, 2017, and Dec 31, 2021. Two participants were unable to receive their assigned regimen for administrative reasons; and 826 participants were included in analyses. Median age was 39 years (IQR 33-46), and 450 (54%) participants were female. Baseline median CD4 count was 206 cells per μL (23-354) and median HIV RNA was 15 400 copies per mL (3600-65 986). The proportion of participants with HIV RNA of less than 50 copies per mL at 48 weeks was 194 (75%) of 257 in the ritonavir-boosted darunavir plus two NRTIs group, 222 (84%) of 264 in the ritonavir-boosted darunavir plus dolutegravir group, and 227 (78%) of 291 in the dolutegravir with tenofovir disoproxil fumarate plus either lamivudine or emtricitabine group. Compared with ritonavir-boosted darunavir plus two NRTIs, the difference in virological suppression was 8·6% (95% CI 1·7 to 15·5; p=0·016) for dolutegravir plus ritonavir-boosted darunavir and 6·7% (-1·2 to 14·4; p=0·093) for dolutegravir with tenofovir disoproxil fumarate plus either lamivudine or emtricitabine. Six deaths occurred, none of which were related to treatment. 19 pregnancies (11 livebirths) occurred with no congenital defects.
Interpretation: In individuals experiencing failure of an NNRTI-based first-line ART, a switch to either dolutegravir plus ritonavir-boosted darunavir or dolutegravir with tenofovir disoproxil fumarate plus either lamivudine or emtricitabine, without universal access to genotyping, was non-inferior in achieving viral suppression compared with ritonavir-boosted darunavir plus two NRTIs. These global data support the most recent WHO treatment guidelines.
Funding: UNITAID; National Institute of Allergy and Infectious Diseases, USA; National Health and Medical Research Council, Australia; ViiV Healthcare; and Janssen.
Copyright © 2024 Elsevier Ltd. All rights reserved, including those for text and data mining, AI training, and similar technologies.
Conflict of interest statement
Declaration of interests GVM, AK, SE, MNP, and MHL received support for the present manuscript from Janssen and ViiV Healthcare, paid to their institution. GVM, AK, and SE received support for the present manuscript from Unitaid, paid to their institution. GVM received support for the present manuscript from the US National Institutes of Health (NIH) and the Australian National Health and Medical Research Council (NHMRC), paid to their institution. MHL received support for the present manuscript from Gilead, paid to their institution. AK received grants or contracts from the Medical Research Future Fund, NHMRC, NIH, and Biotron, paid to their institution; consulting fees from Merck, paid to their institution; support for attending meetings or travel from the HIV Netherlands Australia Thailand Research Collaboration, Keystone conferences, the New South Wales (NSW) Government, and NSW Office for Health and Medical Research, paid to their institution; patent planned issues or pending (PCT/AU2023/050918), with no renumeration; has acted as Chair of the ASCOT data and safety monitoring board, with no renumeration; and is the Director and Chair of Scientia Clinical Research Phase I Unit Board, with no renumeration. ML received fees from Certa Therapeutics for participation on a data safety monitoring board. GVM and MHL have participated on an advisory board for ViiV Healthcare and Gilead. NK received research grants from NIH, WHO, Indian Council of Medical Research, University of New South Wales, Unitaid, Massachusetts General Hospital—Harvard University, and TREAT Asia–The Foundation for AIDS Research for the conduct of research. DB is an employee of ViiV Healthcare and holds GSK stock options. All other authors declare no competing interests.
Figures

References
-
- World Health Organisation. Consolidated guidelines on HIV, viral hepatitis and STI prevention, diagnosis, treatment and care for key populations. 2022. - PubMed
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Guidelines for the Use of Antiretroviral Agents in Adults and Adolescents with HIV. Department of Health and Human Services. 2023. [Available from: https://clinicalinfo.hiv.gov/en/guidelines/adult-and-adolescent-arv..
-
- European AIDS Society EACS Guidelines. 2022. [Available from: https://www.eacsociety.org/media/guidelines-11.1_final_09-10.pdf.
-
- World Health Organization. WHO HIV policy adoption and implementation status in countries. 2023. Fact sheet WHO/UCN/HHS/SIA/2023.02.2023 [Available from: In: https://cdn.who.int/media/docs/default-source/hq-hiv-hepatitis-and-stis-....
-
- Aboud M, Kaplan R, Lombaard J, Zhang F, Hidalgo JA, Mamedova E, et al. Dolutegravir versus ritonavir-boosted lopinavir both with dual nucleoside reverse transcriptase inhibitor therapy in adults with HIV-1 infection in whom first-line therapy has failed (DAWNING): an open-label, non-inferiority, phase 3b trial. Lancet Infect Dis. 2019;19(3):253–64. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
