

Role of tangential biopsy in the diagnosis of nail psoriasis
- PMID: 38789365
- PMCID: PMC11344000
- DOI: 10.1016/j.abd.2023.11.005
Role of tangential biopsy in the diagnosis of nail psoriasis
Abstract
Background: Histopathology can be crucial for diagnosis of inflammatory nail diseases. Longitudinal excision and punch biopsies are the most used techniques to obtain the tissue sample. However, there is a low clinical-histopathological correlation, besides the risk of nail dystrophy. Tangential excision biopsy (TB) is a well-established technique for the investigation of longitudinal melanonychia. TB could also be used to evaluate diseases in which histopathological changes are superficial, as in psoriasis.
Objective: To study the value of TB in the histopathological diagnosis of nail psoriasis.
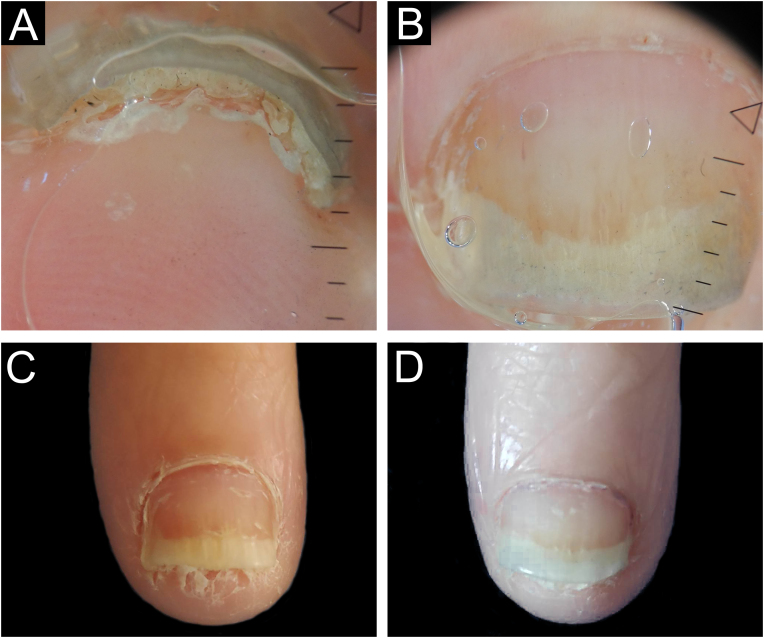
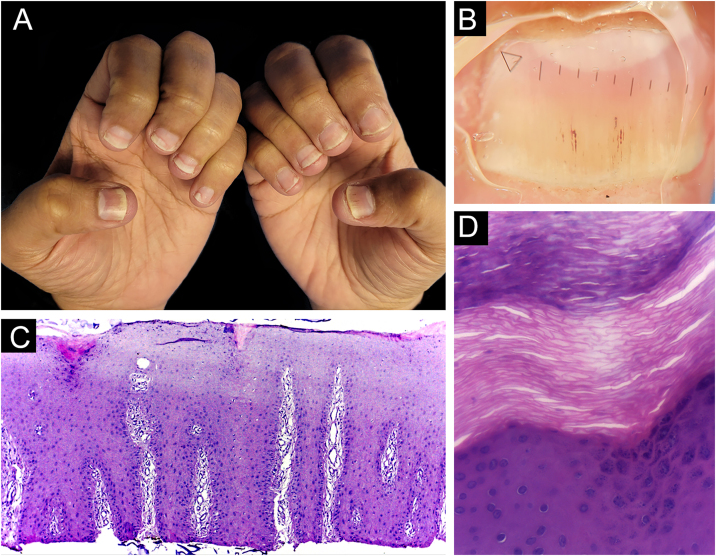
Methods: This is a prospective and descriptive study of the clinical-histopathological findings of samples from the nail bed or matrix and nail plate of 13 patients with clinical suspicion of nail psoriasis. Biopsies were obtained through partial nail avulsion and TB.
Results: In nine patients, the hypothesis of psoriasis was confirmed by histopathology; in one, the criteria for diagnosing nail lichen planus were fulfilled. The tissue sample of only one patient did not reach the dermal papillae, and, in four of 13 patients, the adventitial dermis was not sampled. No patient developed onychodystrophy after the procedure.
Study limitations: In three patients, the clinical and, consequently, histopathological nail changes were subtle. Also, in one patient's TB didn't sample the dermal papillae.
Conclusions: TB is a good option to assist in the histopathological diagnosis of nail psoriasis, especially when appropriate clinical elements are combined. Using this technique, larger and thinner samples, short postoperative recovery time, and low risk of onychodystrophy are obtained.
Keywords: Biopsy; Histopathology; Nail diseases; Psoriasis.
Copyright © 2024 Sociedade Brasileira de Dermatologia. Published by Elsevier España, S.L.U. All rights reserved.
Figures








References
-
- Grover C., Chaturvedi U.K., Reddy B.S. Role of nail biopsy as a diagnostic tool. Indian J Dermatol Venereol Leprol. 2012;78:290–298. - PubMed
-
- Farias D.C., Tosti A., Chiacchio N.D., Hirata S.H. Dermoscopy in nail psoriasis. An Bras Dermatol. 2010;85:101–103. - PubMed
-
- Tan E.S., Chong W.S., Tey H.L. Nail psoriasis: a review. Am J Clin Dermatol. 2012;13:375–388. - PubMed
-
- Hanno R., Mathes B.M., Krull E.A. Longitudinal nail biopsy in evaluation of acquired nail dystrophies. J Am Acad Dermatol. 1986;14:803–809. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
