

Avidity maturation of humoral response following primary and booster doses of BNT162b2 mRNA vaccine among nursing home residents and healthcare workers
- PMID: 38789833
- PMCID: PMC11493945
- DOI: 10.1007/s11357-024-01215-y
Avidity maturation of humoral response following primary and booster doses of BNT162b2 mRNA vaccine among nursing home residents and healthcare workers
Abstract
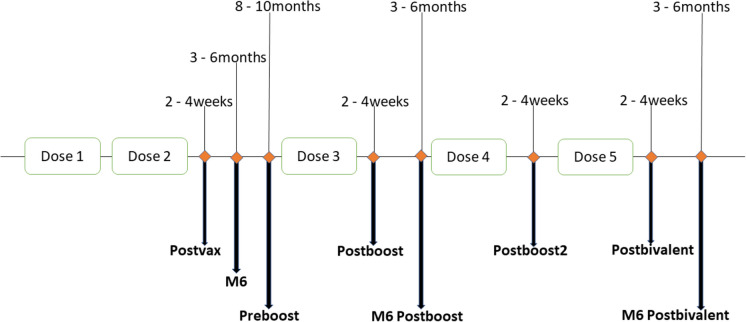
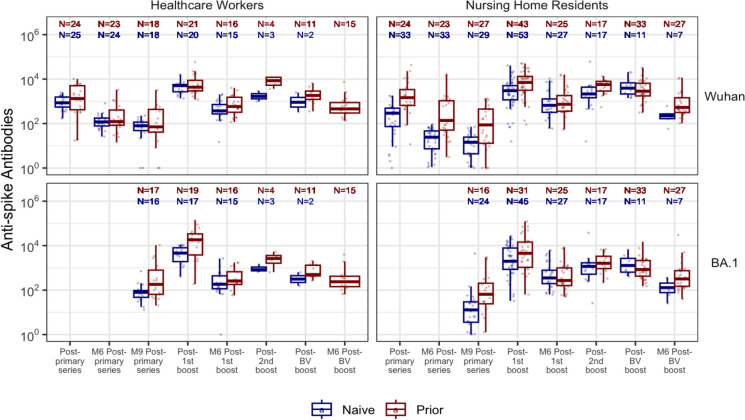
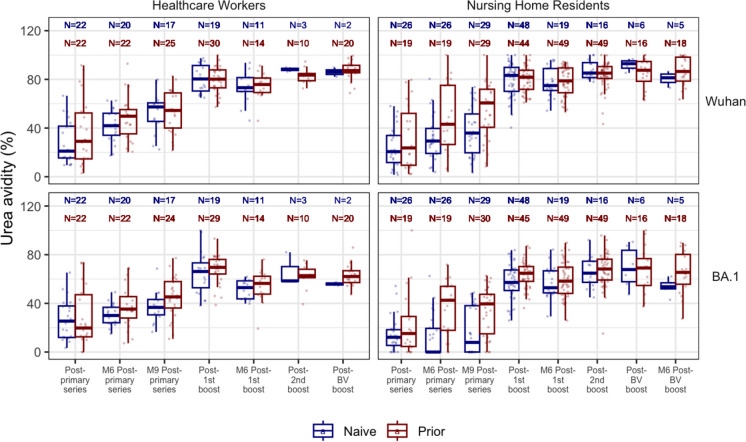
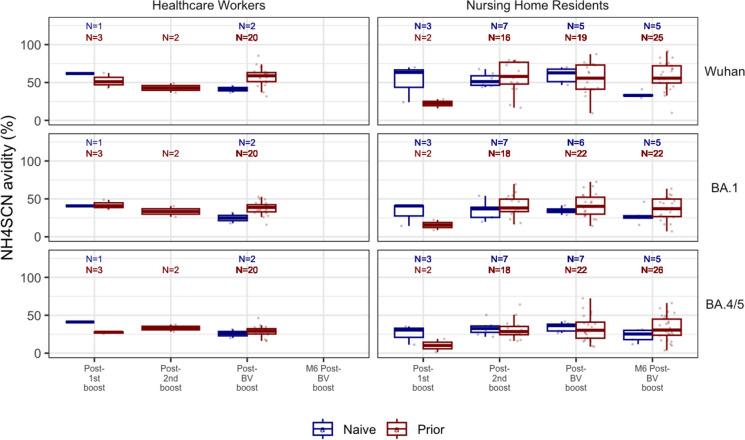
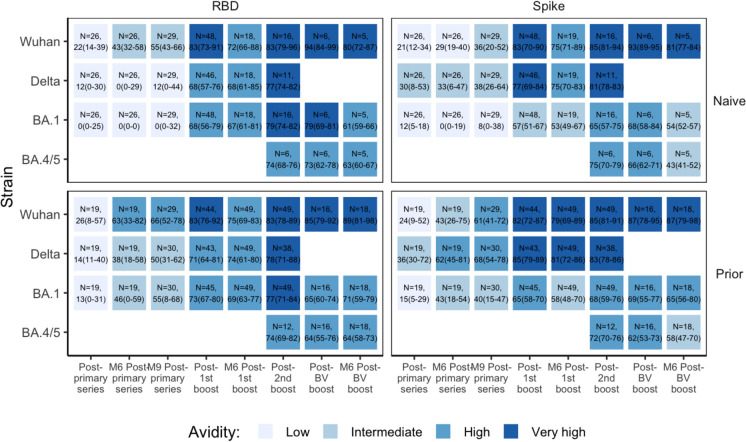
Infections, despite vaccination, can be clinically consequential for frail nursing home residents (NHR). Poor vaccine-induced antibody quality may add risk for such subsequent infections and more severe disease. We assessed antibody binding avidity, as a surrogate for antibody quality, among NHR and healthcare workers (HCW). We longitudinally sampled 112 NHR and 52 HCWs who received the BNT162b2 mRNA vaccine after each dose up to the Wuhan-BA.4/5-based Omicron bivalent boosters. We quantified anti-spike, anti-receptor binding domain (RBD), and avidity levels to the ancestral Wuhan, Delta, and Omicron BA.1 & 4/5 strains. The primary vaccination series produced substantial anti-spike and RBD levels which were low in avidity against all strains tested. Antibody avidity progressively increased in the 6-8 months that followed. Avidity significantly increased after the 1st booster but not for subsequent boosters. This study underscores the importance of booster vaccination among NHR and HCWs. The 1st booster dose increases avidity, increasing vaccine-induced functional antibody. The higher cross-reactivity of higher avidity antibodies to other SARS-CoV-2 strains should translate to better protection from ever-evolving strains. Higher avidities may help explain how the vaccine's protective effects persist despite waning antibody titers after each vaccine dose.
Keywords: Affinity maturation; Avidity; BNT162b2 mRNA vaccine; Bivalent boosters; COVID-19; Healthcare workers; Nursing home residents; Omicron.
© 2024. This is a U.S. Government work and not under copyright protection in the US; foreign copyright protection may apply.
Conflict of interest statement
Stefan Gravenstein (S. G.) and David H. Canaday (D. H. C.) are recipients of investigator-initiated grants to their universities from Pfizer to study pneumococcal vaccines, Moderna to study respiratory infection surveillance, and Sanofi Pasteur and Seqirus to study influenza vaccines, and S.G. from Genentech on influenza antivirals. S. G. also receives consulting fees from GlaxoSmithKline, Icosavax, Janssen, Merck, Moderna, Novavax, Pfizer, Reviral, Sanofi, Seqirus, and Vaxart, and has received fees for speaking for Janssen, Moderna, Sanofi, and Seqirus.
Figures
References
-
- Nanduri S, Pilishvili T, Derado G, et al. Effectiveness of Pfizer-BioNTech and Moderna Vaccines in Preventing SARS-CoV-2 Infection Among Nursing Home Residents Before and During Widespread Circulation of the SARS-CoV-2 B.1.617.2 (Delta) Variant — National Healthcare Safety Network, March 1–August 1, 2021. MMWR Morb Mortal Wkly Rep. 2021;70:1163–6. 10.15585/mmwr.mm7034e3. - PMC - PubMed
-
- Nilsson L, Andersson C, Kastbom L, Sjödahl R. Association between vaccination and preventive routines on COVID-19-related mortality in nursing home facilities: a population-based systematic retrospective chart review. Prim Health Care Res Dev. 2022;18(23): e75. 10.1017/S1463423622000640. - PMC - PubMed
-
- Canaday DH, Oyebanji OA, Keresztesy D, et al. Significant reduction in vaccine-induced antibody levels and neutralization activity among healthcare workers and nursing home residents 6 months following coronavirus disease 2019 BNT162b2 mRNA vaccination. Clin Infect Dis. 2022;75(1):e884–7. 10.1093/cid/ciab963. - PMC - PubMed
-
- Lustig Y, Gonen T, Meltzer L, et al. Superior immunogenicity and effectiveness of the third compared to the second BNT162b2 vaccine dose. Nat Immunol. 2022. 10.1038/s41590-022-01212-3. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
