

Time to improvement of pain, morning stiffness, fatigue, and disease activity in patients with ankylosing spondylitis treated with tofacitinib: a post hoc analysis
- PMID: 38790040
- PMCID: PMC11127290
- DOI: 10.1186/s13075-024-03313-w
Time to improvement of pain, morning stiffness, fatigue, and disease activity in patients with ankylosing spondylitis treated with tofacitinib: a post hoc analysis
Abstract
Background: Tofacitinib is an oral Janus kinase inhibitor for treatment of ankylosing spondylitis (AS). Time to improvement in core domains of AS was estimated in tofacitinib-treated patients with AS.
Methods: This post hoc analysis used phase 3 trial data from patients with AS receiving tofacitinib 5 mg twice daily or placebo to week (W)16; all patients received open-label tofacitinib W16-48.
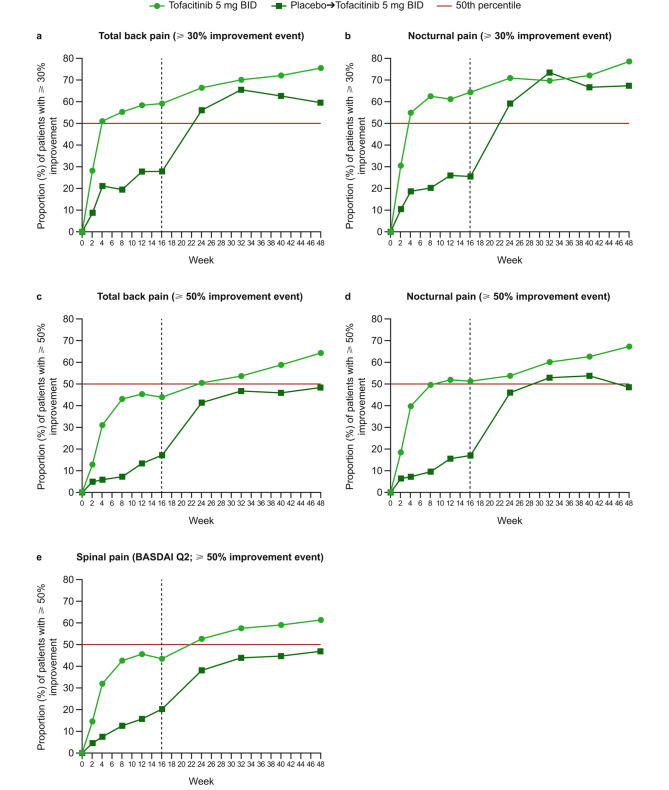
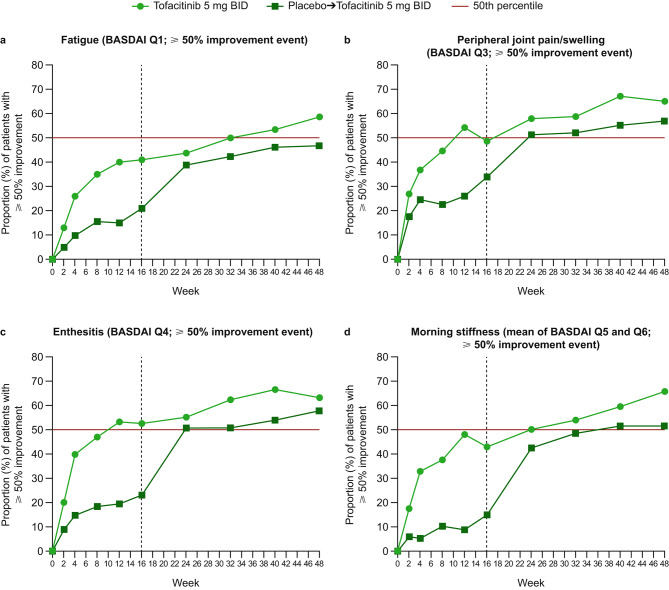
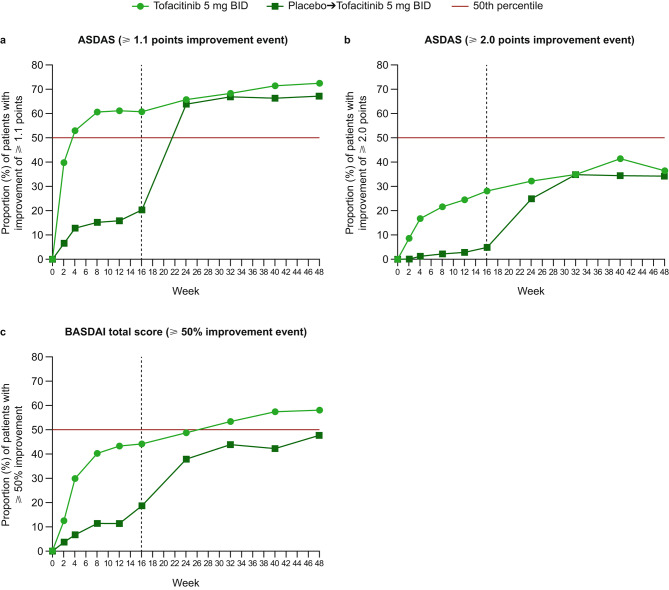
Outcomes: nocturnal pain; total back pain; fatigue, spinal pain, peripheral joint pain/swelling, enthesitis, and morning stiffness (Bath AS Disease Activity Index [BASDAI] questions 1-6); BASDAI total score; AS Disease Activity Score (ASDAS). Median time to improvement events was estimated using non-parametric Kaplan-Meier models. Improvement events were defined as initial (first post-baseline observation) and continued (sustained for 2 consecutive visits) ≥ 30% and ≥ 50% improvement in back/nocturnal pain or BASDAI questions/total scores, or ASDAS improvement ≥ 1.1 and ≥ 2.0 points.
Results: 269 patients (tofacitinib: n = 133; placebo-to-tofacitinib: n = 136) were assessed. Median time to improvement was shorter, and more patients experienced improvements with tofacitinib vs. placebo-to-tofacitinib; differences observed from W2 (first post-baseline assessment). Median time to initial (continued) ≥ 30% pain improvement was 4 (4-8) weeks for tofacitinib vs. 24 (24) weeks for placebo-to-tofacitinib (8 [8] weeks post-switch). Median time to initial (continued) ≥ 50% improvement of pain, peripheral joint pain/swelling and enthesitis, morning stiffness, BASDAI total score, and fatigue was 8-24 (12-40) weeks with tofacitinib vs. 24-32 weeks (32 weeks-not estimable [NE]) with placebo-to-tofacitinib. Median time to initial (continued) ASDAS improvement ≥ 1.1 points was 4 (8) weeks for tofacitinib vs. 24 (24) weeks for placebo-to-tofacitinib, and NE for improvement ≥ 2.0 points with either treatment.
Conclusions: Improvements in AS core domains occurred more rapidly with tofacitinib vs. placebo-to-tofacitinib. Half of tofacitinib-treated patients with AS will likely experience improvements ≥ 30% in pain and ≥ 1.1 points in ASDAS during month (M)1, ≥ 50% improvement in nocturnal pain and enthesitis by M2, and in morning stiffness by M3. Results show that initiating tofacitinib as soon as possible is associated with quicker improvements in AS core domains vs. delaying treatment.
Trial registration: ClinicalTrials.gov, NCT03502616, 11 April 2018.
Keywords: Ankylosing spondylitis; Disease activity; Fatigue; Pain; Patient-reported outcomes; Spondyloarthritis; Tofacitinib.
© 2024. Pfizer Inc and Navarro-Compán, Deodhar, Bahiri.
Conflict of interest statement
VN-C has received grant/research support from AbbVie and Novartis, has acted as a consultant/speaker for, or has received honoraria from, AbbVie, Eli Lilly, Fresenius Kabi, Janssen, MoonLake, MSD, Novartis, Pfizer Inc, and UCB. AD has received grant/research support from AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, Galvani, Janssen, Novartis, Pfizer Inc, and UCB, has acted as a consultant for AbbVie, Bristol Myers Squibb, Celgene, Eli Lilly, GSK, Janssen, MoonLake, Novartis, Pfizer Inc, and UCB, and has acted as a speaker for, or has received honoraria from, Eli Lilly, Janssen, Novartis, Pfizer Inc, and UCB. RB has received grant/research support from AbbVie, Janssen, Novartis, and Pfizer Inc, has acted as a consultant for AbbVie, Pfizer Inc, and Roche, has acted as a speaker for, or has received honoraria from, AbbVie, Cooper Maroc, Hikma, Janssen, Novartis, Pfizer Inc, Phi, Roche, and Sothema, and has been an advisor or review panel member for AbbVie, Janssen, Hikma, Newbridge, Novartis, Pfizer Inc, Roche, and Sothema. AGB, JCC, and JR are employees and stockholders of Pfizer Inc.
Figures
References
-
- Bohn R, Cooney M, Deodhar A, Curtis JR, Golembesky A. Incidence and prevalence of axial spondyloarthritis: methodologic challenges and gaps in the literature. Clin Exp Rheumatol. 2018;36:263–74. - PubMed
-
- Žagar I, Delimar V, Čota S, Špoljarić Carević S, Kovač Durmiš K, Laktašić Žerjavić N, et al. The impact of disease activity on quality of life, fatigue, functional status and physical activity in patients with ankylosing spondylitis. Psychiatr Danub. 2021;33(Suppl 4):1278–83. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
