

The Interplay between Perioperative Oxidative Stress and Hepatic Dysfunction after Human Liver Resection: A Prospective Observational Pilot Study
- PMID: 38790695
- PMCID: PMC11118143
- DOI: 10.3390/antiox13050590
The Interplay between Perioperative Oxidative Stress and Hepatic Dysfunction after Human Liver Resection: A Prospective Observational Pilot Study
Abstract
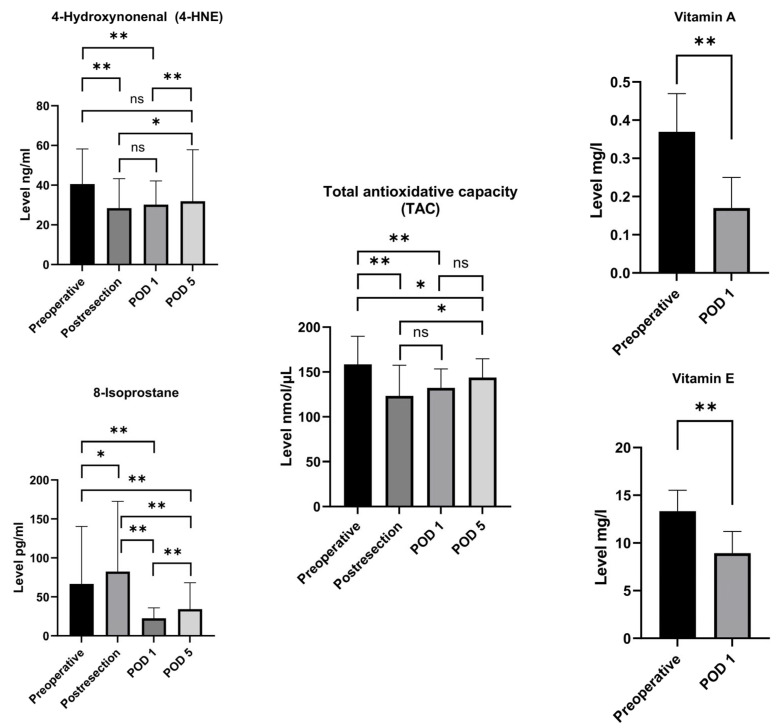
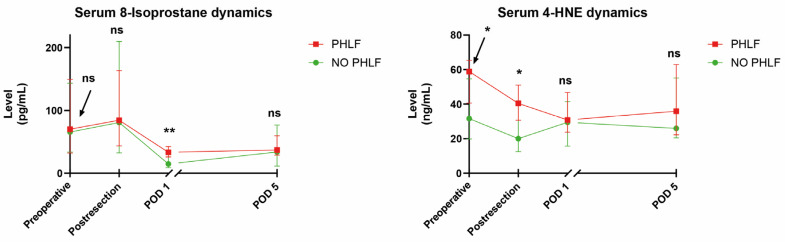
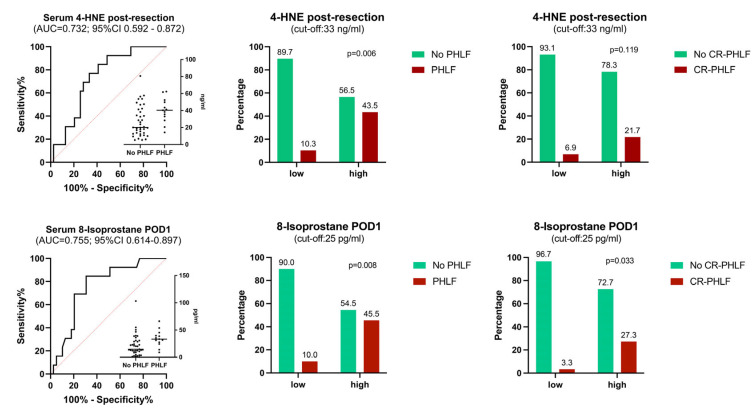
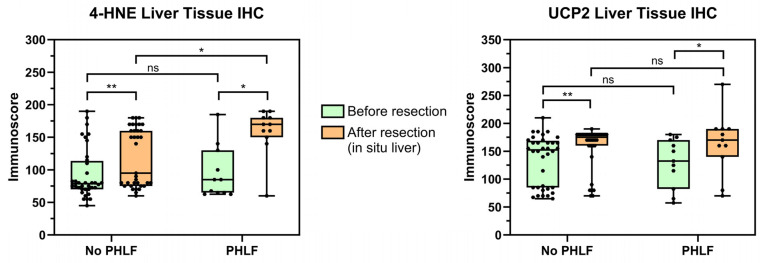
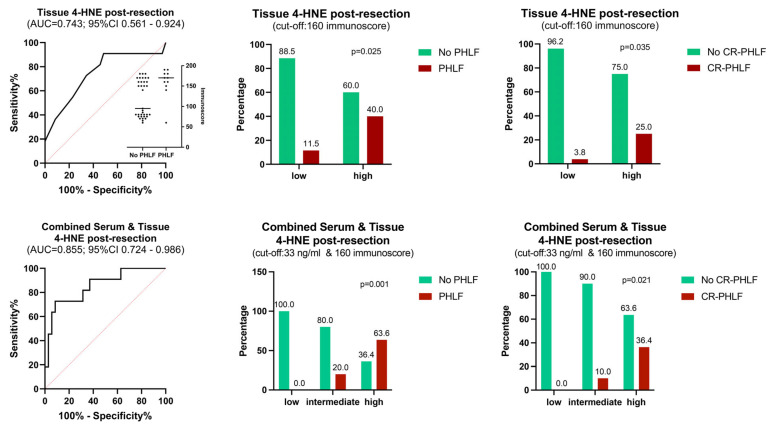
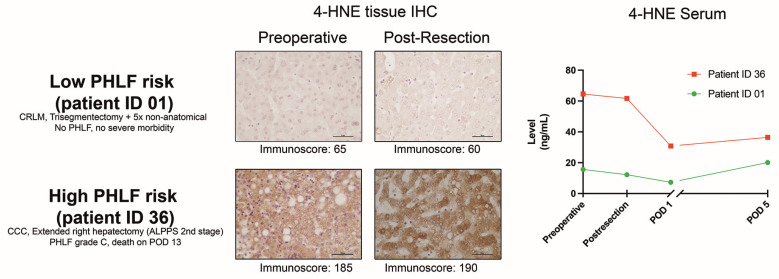
Post-hepatectomy liver failure (PHLF) remains the major contributor to death after liver resection. Oxidative stress is associated with postoperative complications, but its impact on liver function is unclear. This first in-human, prospective, single-center, observational pilot study evaluated perioperative oxidative stress and PHLF according to the ISGLS (International Study Group for Liver Surgery). Serum 8-isoprostane, 4-hydroxynonenal (4-HNE), total antioxidative capacity, vitamins A and E, and intraoperative, sequential hepatic tissue 4-HNE and UCP2 (uncoupling protein 2) immunohistochemistry (IHC) were assessed. The interaction with known risk factors for PHLF and the predictive potential of oxidative stress markers were analyzed. Overall, 52 patients were included (69.2% major liver resection). Thirteen patients (25%) experienced PHLF, a major factor for 90-day mortality (23% vs. 0%; p = 0.013). Post-resection, pro-oxidative 8-isoprostane significantly increased (p = 0.038), while 4-HNE declined immediately (p < 0.001). Antioxidative markers showed patterns of consumption starting post-resection (p < 0.001). Liver tissue oxidative stress increased stepwise from biopsies taken after laparotomy to post-resection in situ liver and resection specimens (all p < 0.001). Cholangiocarcinoma patients demonstrated significantly higher serum and tissue oxidative stress levels at various timepoints, with consistently higher preoperative values in advanced tumor stages. Combining intraoperative, post-resection 4-HNE serum levels and in situ IHC early predicted PHLF with an AUC of 0.855 (63.6% vs. 0%; p < 0.001). This was also associated with grade B/C PHLF (36.4% vs. 0%; p = 0.021) and 90-day mortality (18.2% vs. 0%; p = 0.036). In conclusion, distinct patterns of perioperative oxidative stress levels occur in patients with liver dysfunction. Combining intraoperative serum and liver tissue markers predicts subsequent PHLF. Cholangiocarcinoma patients demonstrated pronounced systemic and hepatic oxidative stress, with increasing levels in advanced tumor stages, thus representing a worthwhile target for future exploratory and therapeutic studies.
Keywords: liver dysfunction; liver resection; outcome; oxidative stress; post-hepatectomy liver failure.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
LinkOut - more resources
Full Text Sources
