

Rebound Acid Hypersecretion after Withdrawal of Long-Term Proton Pump Inhibitor (PPI) Treatment-Are PPIs Addictive?
- PMID: 38791497
- PMCID: PMC11122117
- DOI: 10.3390/ijms25105459
Rebound Acid Hypersecretion after Withdrawal of Long-Term Proton Pump Inhibitor (PPI) Treatment-Are PPIs Addictive?
Abstract
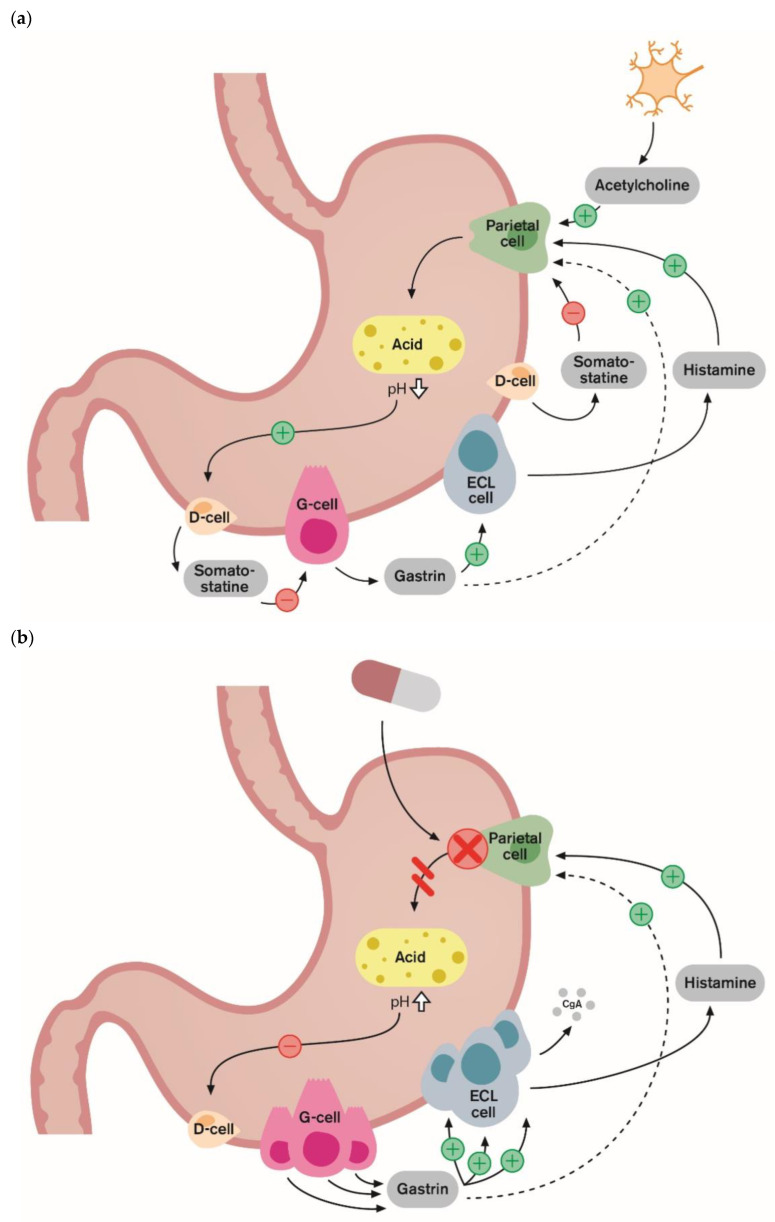
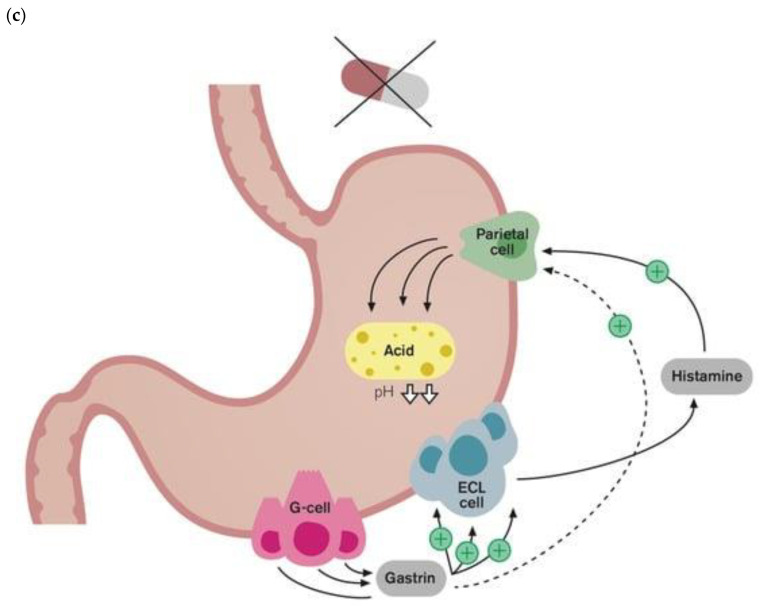
Proton pump inhibitors (PPIs) are widely used in the long-term treatment of gastroesophageal reflux disease (GERD) and other upper gastrointestinal disorders, such as the healing of peptic ulcers and/or prophylactic treatment of peptic ulcers. PPIs are also widely used as symptomatic treatment in patients with functional dyspepsia. One of the adverse effects of the long-term use of PPI is rebound acid hypersecretion (RAHS), which can occur after the withdrawal of PPI therapy due to a compensatory increase in gastric acid production. Mechanisms of the RAHS have been well established. Studies have shown that pentagastrin-stimulated acid secretion after the discontinuation of PPIs increased significantly compared to that before treatment. In healthy volunteers treated with PPIs, the latter induced gastrointestinal symptoms in 40-50% of subjects after the discontinuation of PPI therapy but after stopping the placebo. It is important for practicing physicians to be aware and understand the underlying mechanisms and inform patients about potential RAHS before discontinuing PPIs in order to avoid continuing unnecessary PPI therapy. This is important because RAHS may lead patients to reuptake PPIs as symptoms are incorrectly thought to originate from the recurrence of underlying conditions, such as GERD. Mechanisms of RAHS have been well established; however, clinical implications and the risk factors for RAHS are not fully understood. Further research is needed to facilitate appropriate management of RAHS in the future.
Keywords: discontinuation; gastrin; proton pump inhibitors; rebound acid hypersecretion; withdrawal.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
